













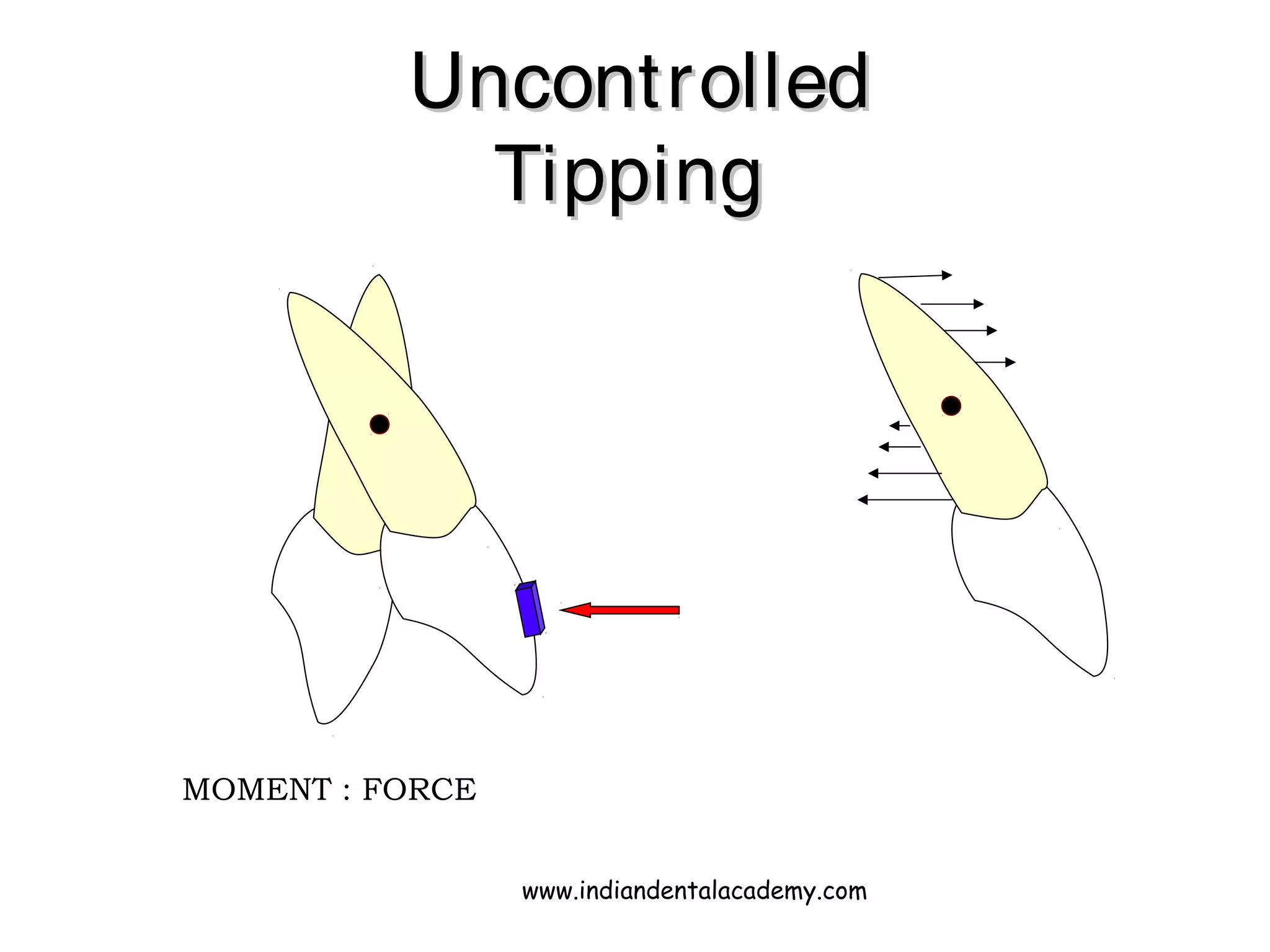
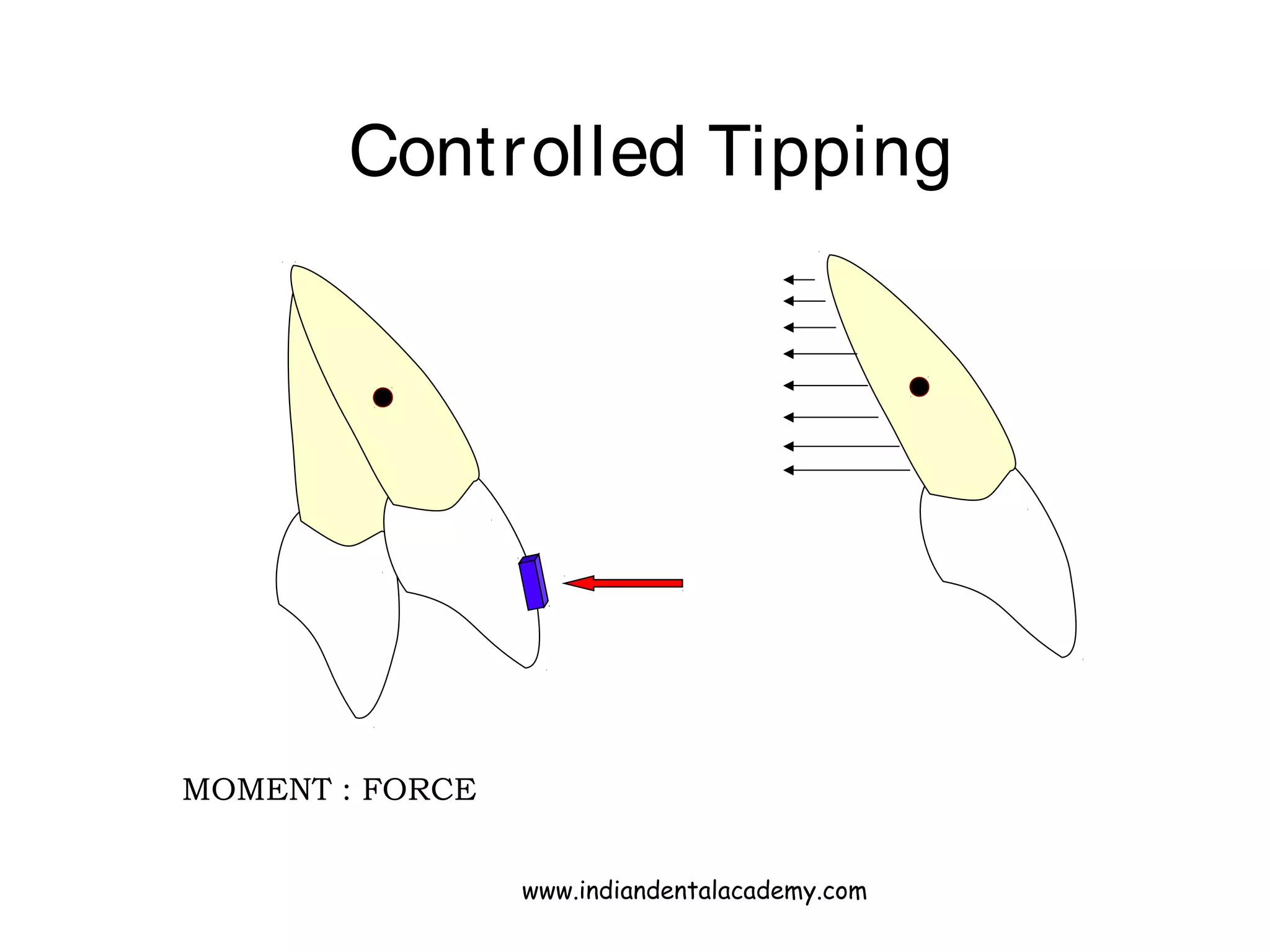

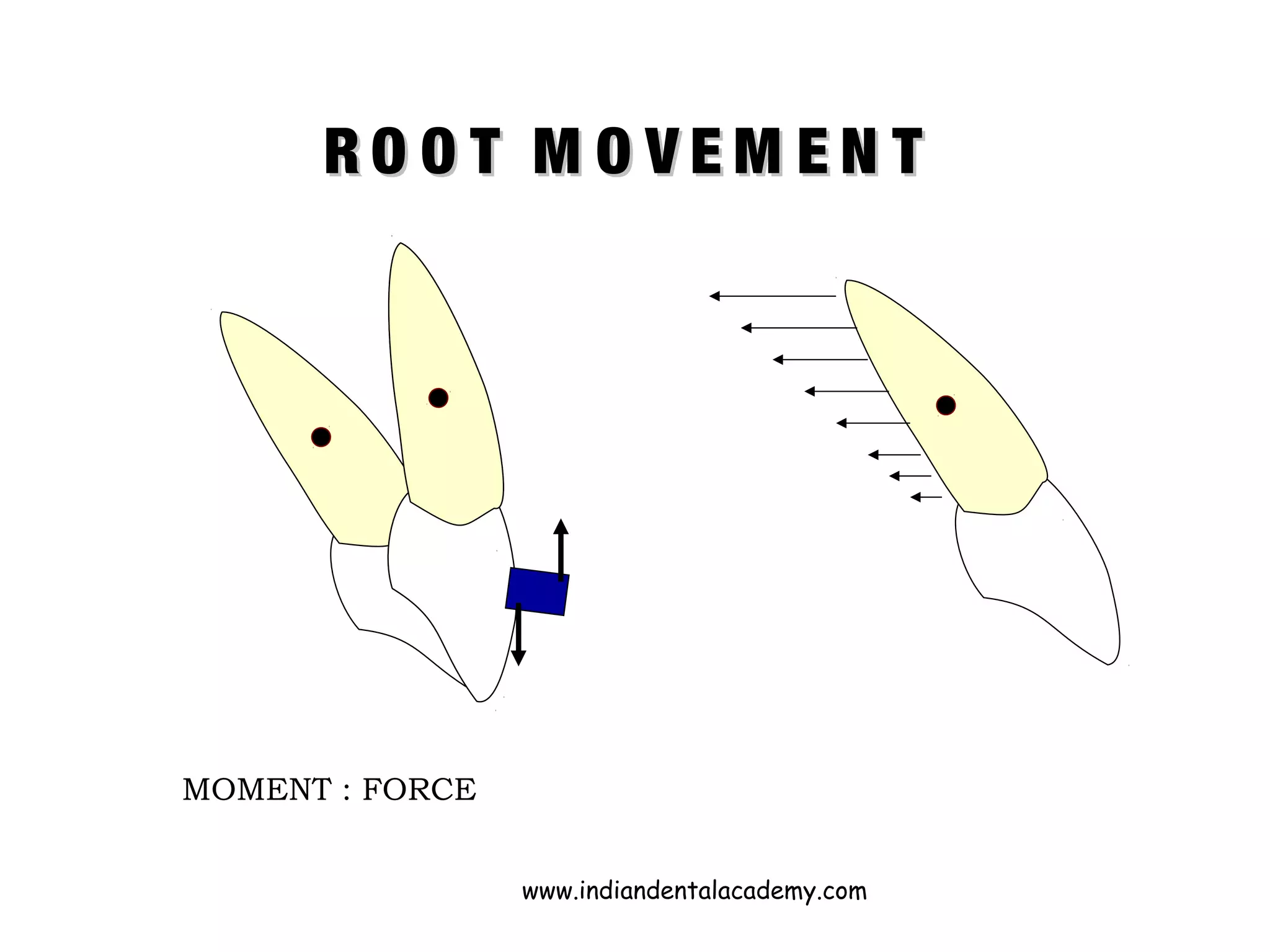
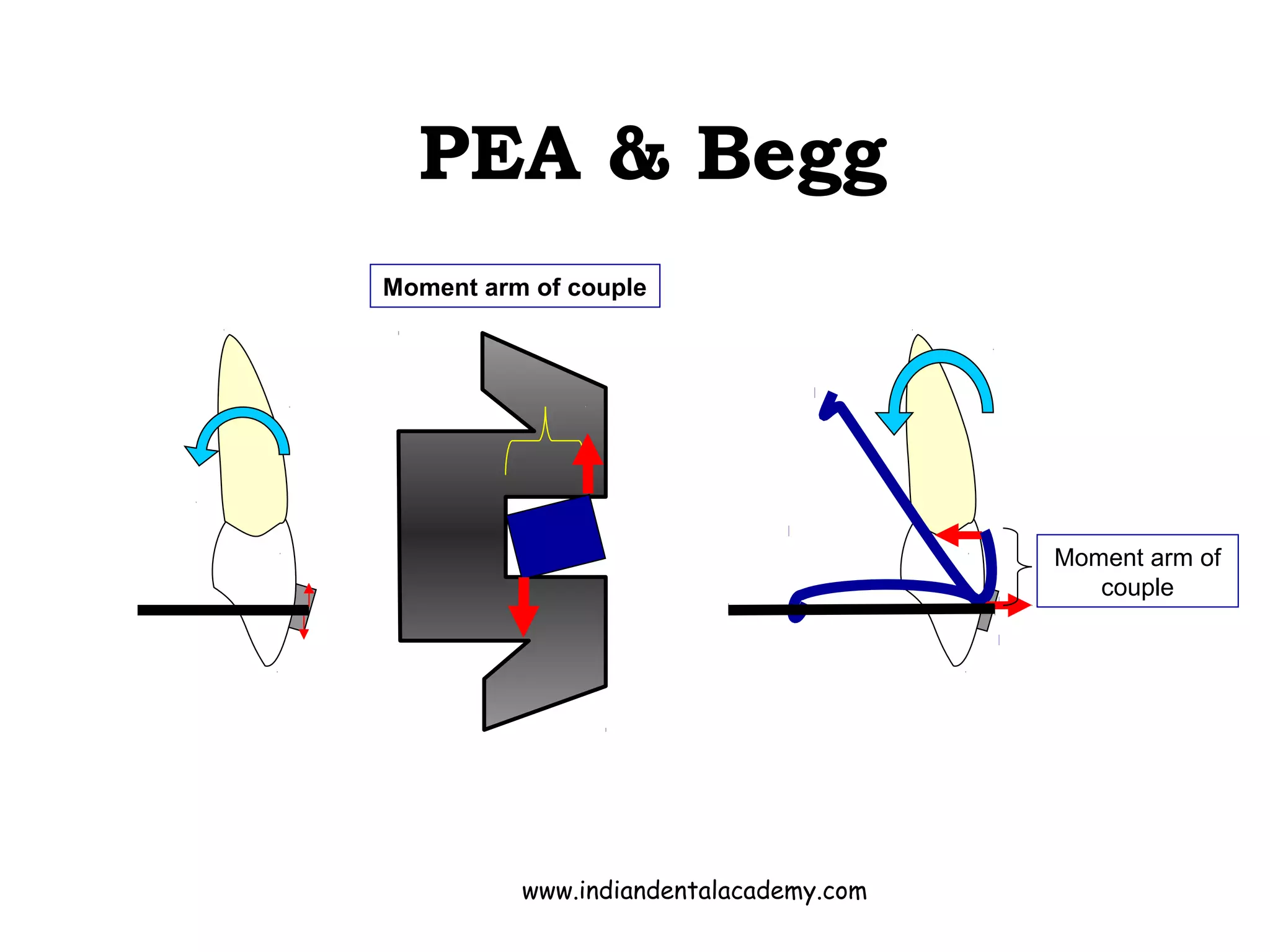






































The document discusses the importance of root movement in orthodontics, emphasizing the control of axial inclinations for achieving stable treatment results. It covers various techniques and biomechanical considerations involved in root correction and the evaluation of tooth positions during treatment. Multiple methodologies and tools are outlined to facilitate effective root movement in both fixed and removable appliances.











































































































