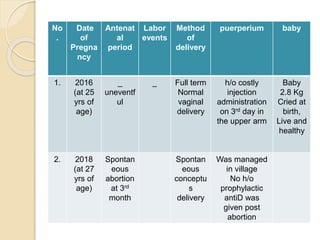
The document presents a case of a 29-year-old multigravida woman, currently 10 weeks and 1 day pregnant, with blood group B-negative married to a B-positive husband. She has a history of one first trimester abortion and is asymptomatic during this antenatal visit. Examination reveals mild pallor but no significant abnormalities, raising concerns about potential Rh incompatibility in the current pregnancy.