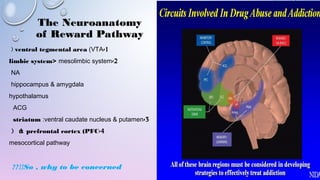
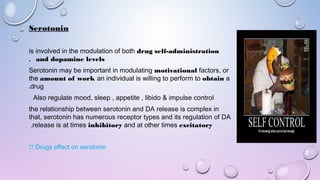
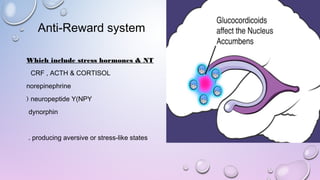
1) The document discusses the neuroanatomy and neurophysiology of the brain's reward pathway, which is centered around dopamine release in the ventral tegmental area and nucleus accumbens. Drugs of abuse hijack this pathway, flooding it with unnaturally high levels of dopamine.
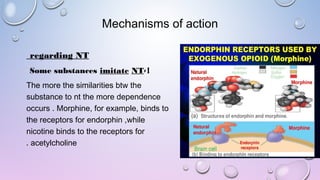
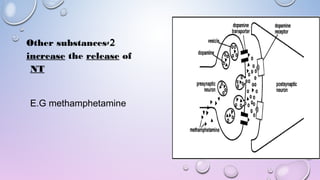
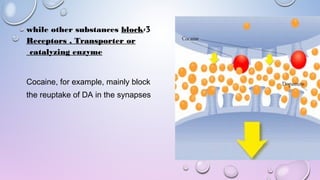
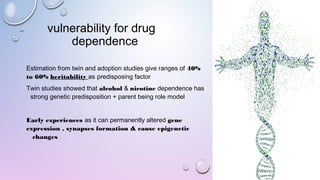
2) Mechanisms of drug action involve mimicking neurotransmitters like opioids mimicking endorphins, or blocking reuptake of neurotransmitters like cocaine blocking dopamine reuptake. This leads to long-lasting changes in gene expression and synaptic plasticity.
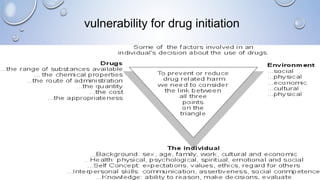
3) Vulnerability to drug dependence involves genetic and environmental factors like trauma or mental health issues that may lead to self-medication. Relapse is driven

































































![CTEV [ clubfoot] DR ARUN LAL ,DR MOHAMED ASHRAF travancore medical college k...](https://cdn.slidesharecdn.com/ss_thumbnails/ctevclubfootdrarunlaldrmohamedashraftravancoremedicalcollegekollamkeralaindia-260208063247-18fc466c-thumbnail.jpg?width=640&height=640&fit=bounds)






