Downloaded 55 times
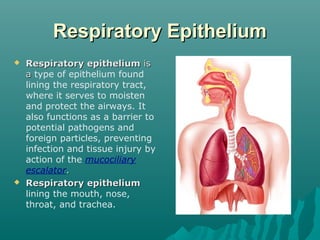
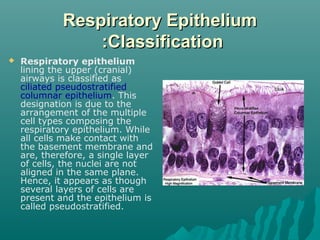
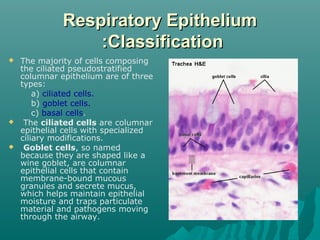
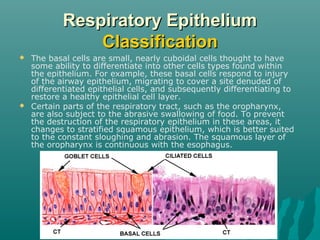

The respiratory epithelium lines the respiratory tract from the nose to the trachea. It is classified as ciliated pseudostratified columnar epithelium in the upper airways, composed mainly of ciliated cells, goblet cells, and basal cells. The cilia beat in a coordinated way to move mucus up the airways via the mucociliary escalator, trapping pathogens and particles to be expelled or swallowed, protecting the lungs.