
Recommended
Recommended
More Related Content
Similar to RePrefElia NuLeveb Coc Ded SchIntern.docx
Similar to RePrefElia NuLeveb Coc Ded SchIntern.docx (15)
More from sodhi3
More from sodhi3 (20)
Recently uploaded
Recently uploaded (20)
RePrefElia NuLeveb Coc Ded SchIntern.docx
- 1. Re Pr ef Eli a Nu Leve b Co c De d Sch International Journal of Nursing Studies 49 (2012) 345–359 A R Artic Rece Rece Acce Keyw Pres Prev Revi
- 2. Hos Met § pub doi: * 002 doi: view eventing pressure ulcers—Are pressure-redistributing support surfaces fective? A Cochrane systematic review and meta-analysis§ zabeth McInnes a,*, Asmara Jammali-Blasi a, Sally Bell-Syer b, Jo Dumville c, Nicky Cullum d rsing Research Institute – St Vincents and Mater Health Sydney & Australian Catholic University, National Centre for Clinical Outcomes Research (NaCCOR), l 5, Delacy Building, 379 Victoria St Darlinghurst, NSW 2010, Australia chrane Wounds Group, Department of Health Sciences, University of York, Heslington, York YO10 5DD, UK partment of Health Sciences, University of York, Heslington, York YO10 5DD, UK
- 3. ool of Nursing, Midwifery and Social Work, University of Manchester, Room 6.326, Jean McFarlane Building, Oxford Road, Manchester M13 9PL, UK What is already known about this topic? � Pressure ulcers are areas of localised damage to the skin and underlying tissue due to pressure, shear or friction. � Pressure ulcers may affect those who are medically compromised, obese, pregnant and the elderly. T I C L E I N F O le history: ived 27 July 2011 ived in revised form 11 October 2011 pted 18 October 2011 ords: sure ulcer ention ew pital equipment a-analysis A B S T R A C T
- 4. Objectives: To undertake a systematic review of the effectiveness of pressure redistributing support surfaces in the prevention of pressure ulcers. Design: Systematic review and meta-analysis. Data sources: Cochrane Wound Group Specialised Register, The Cochrane Central Register of Controlled Trials, Ovid MEDLINE, Ovid EMBASE and EBSCO CINAHL. The reference sections of included trials were searched for further trials. Review methods: Randomised controlled trials and quasi- randomised trials, published or unpublished, which assessed the effects of support surfaces in preventing pressure ulcers (of any grade), in any patient group, in any setting compared to any other support surface, were sought. Two reviewers extracted and summarised details of eligible trials using a standardised form and assessed the methodological quality of each trial using the Cochrane risk of bias tool. Results: Fifty-three eligible trials were identified with a total of 16,285 study participants.
- 5. Overall the risk of bias in the included trials was high. Pooled analysis showed that: (i) foam alternatives to the standard hospital foam mattress reduce the incidence of pressure ulcers in people at risk (RR 0.40, 95% CI 0.21–0.74) and Australian standard medical sheepskins prevent pressure ulcers compared to standard care (RR 0.48, 95% CI 0.31–0.74). Pressure-redistributing overlays on the operating table compared to standard care reduce postoperative pressure ulcer incidence (RR 0.53, 95% CI 0.33– 0.85). Conclusions: While there is good evidence that higher specification foam mattresses, sheepskins, and that some overlays in the operative setting are effective in preventing pressure ulcers, there is insufficient evidence to draw conclusions on the value of seat cushions, limb protectors and various constant low pressure devices. The relative merits of higher-tech constant low pressure and alternating pressure for prevention are unclear. More robust trials are required to address these research gaps. � 2011 Elsevier Ltd. All rights reserved.
- 6. This review is an abridged version of a Cochrane Review previously lished in the Cochrane Database of Systematic Reviews 2011, Issue 4, 10.1002/14651858.CD001735. Corresponding author. Tel.: +61 02 8382 3793; fax: +61 02 8382 3792. E-mail address: [email protected] (E. McInnes). Contents lists available at SciVerse ScienceDirect International Journal of Nursing Studies journal homepage: www.elsevier.com/ijns 0-7489/$ – see front matter � 2011 Elsevier Ltd. All rights reserved. 10.1016/j.ijnurstu.2011.10.014 http://dx.doi.org/10.1016/j.ijnurstu.2011.10.014 mailto:[email protected] http://www.sciencedirect.com/science/journal/00207489 http://dx.doi.org/10.1016/j.ijnurstu.2011.10.014 E. McInnes et al. / International Journal of Nursing Studies 49 (2012) 345–359346 � Clinical and non-clinical settings use a variety of support surfaces to prevent the occurrence of pressure ulcers. What this paper adds � Low-tech foam mattresses, sheepskins and operating
- 7. table overlays are able to prevent pressure ulcers. � There is insufficient evidence to draw conclusions on the value of seat cushions, limb protectors and various constant low pressure devices. � Future trials investigating the effectiveness of support surfaces for preventing pressure ulcers should be robustly designed, paying particular attention to report- ing follow-up times; attrition rates, intention to treat analysis, and giving adequate descriptions of interven- tions, comparators and definitions of pressure ulcer status. 1. Introduction Rationale: Pressure ulcers (also known as pressure sores, bed sores and decubitus ulcers) are chronic wounds involving areas of localised damage to the skin and underlying tissue, which are caused by pressure, or caused by both pressure and shear (European Pressure Ulcer Advisory Panel and National Pressure Ulcer Advisory Panel, 2009). Pressure ulcers may develop in those who are seriously ill, neurologically compromised, or who have impaired mobility (Allman, 1997; Berlowitz et al., 1997; Bianchetti et al., 1993). Poor nutrition (Banks, 1998; Casey, 1998, 1997), obesity (Gallagher, 1997), poor posture and age (Rinda and Falce, 2002; Spoelhof, 2000; Thomas, 2001) have also been reported as increasing the risk of developing pressure ulcers. Studies conducted in health- care facilities in Europe, Canada and the USA, report pressure ulcer prevalence ranges of 8–26% (Vanderwee et al., 2007a; Woodbury and Houghton, 2004). In Australia a national prevalence rate of 5–15% has been reported (Australian Commission for Safety and Quality in Health Care (ACSQHC), 2005). In Europe 58% of pressure ulcers
- 8. and 70% in the USA are classified as Grade 2 and above (Vanderwee et al., 2007b; Van Gilder et al., 2009). A Grade 2 pressure ulcer involves partial thickness loss of the dermis and a pressure ulcer classified as Grade 2 or greater is a serious pressure injury requiring treatment (European Pressure Ulcer Advisory Panel and National Pressure Ulcer Advisory Panel, 2009). There is some evidence that different grades of ulcer have different aetiologies and it is suggested that Grade 2 ulcers are due to friction and Grades 3 and 4 due to pressure and shearing forces (Lahmann and Kottner, 2011). Pressure ulcers are debilitating, painful and difficult to heal (Girouard et al., 2008). They are also associated with psychological, physical and social problems (Fox, 2002; Franks et al., 2002; Langemo et al., 2000), and have a detrimental impact on quality of life (Essex et al., 2009; Gorecki et al., 2009). The costs of preventing and treating pressure ulcers are high. Total annual costs for treating pressure ulcers in the UK have been estimated at between 1.4 and 2.1 billion pounds (Phillips and Buttery, 2009) and in the USA between 2.2 and 3.6 billion dollars (Van Gilder et al., 2009). In Australia, the predicted number of bed days lost due to pressure ulcers incurred a median opportunity cost of AU$285 million (Graves et al., 2005a) and a median excess length of stay of 4.31 days (Graves et al., 2005b). The management of pressure ulcers is challenging for clinicians (Fox, 2002; Franks et al., 2002; Langemo et al., 2000) and pressure-redistributing support surfaces are commonly used as a means of prevention. Pressure redistributing support surfaces aim to reduce the magni- tude and/or duration of pressure between an individual and the support surface used (interface pressure) in order to prevent or treat the pressure ulcer (European Pressure
- 9. Ulcer Advisory Panel and National Pressure Ulcer Advisory Panel, 2009). Support surfaces include overlays, mat- tresses, cushions, sheepskins and beds. These can be classified either as ‘low tech’ devices, which are conform- ing support surfaces that mould around the shape of the patient to distribute the body weight over a large area and include constant low-pressure devices such as foam mattresses, or ‘high tech’ dynamic devices, such as alternating support surfaces where inflatable cells alter- nately inflate and deflate (McInnes et al., 2011). Some support surfaces such as turning beds/frames are mechan- ical and work by motor-driven turning and tilting. There are many such support surfaces available and prevention initiatives should be based on the best available evidence of effectiveness. Hence we have undertaken a systematic review of randomised controlled trials (RCTs) with the aim of providing clinicians with information on which to base decisions about choice of support surfaces for the prevention of pressure ulcers. Objective: To examine (1) which pressure-redistributing cushions, beds, mattress overlays and mattress replace- ments reduce the incidence of pressure ulcers compared with standard support surfaces and (2) how effective different pressure-redistributing surfaces are in preventing pressure ulcers, when compared with one another. 2. Methods Protocol and registration: The full Cochrane systematic review on which this article is based can be accessed from the Cochrane Database of Systematic Reviews (report number CD001735) (McInnes et al., 2011). This report adheres to the PRISMA method for reporting on systematic reviews (Moher et al., 2009).
- 10. Eligibility criteria: RCTs and quasi-randomised trials comparing beds, mattresses, mattress overlays and cush- ions in any setting, on any clinical population, of any age, with any condition, which measured the incidence of new pressure ulcers. Trials which used only subjective mea- sures of outcome (e.g. skin condition ‘‘better’’ or ‘‘worse’’) were excluded, as were trials which reported only proxy outcome measures such as interface pressure. Search Strategy (including information sources): We searched, without language, publication status or date restriction, the Cochrane Wounds Group Specialised Register (searched 8 December 2010); The Cochrane Central Register of Controlled Trials (CENTRAL) (The Cochrane Library Issue 4, 2010); Ovid MEDLINE (1950 to November Week 3, 2010); Ovid MEDLINE In-Process and Oth EM to com Stra sen sion CIN dev wo 200 Coc pre we pub
- 13. # E. McInnes et al. / International Journal of Nursing Studies 49 (2012) 345–359 347 er Non-Indexed Citations (December 07, 2010); Ovid BASE (1980–2010 Week 48) and EBSCO CINAHL (1982 3 December 2010). The Ovid MEDLINE search was bined with the Cochrane Highly Sensitive Search tegy for identifying randomised trials in MEDLINE: sitivity- and precision-maximising version (2008 revi- ) (Lefebvre et al., 2009). The Ovid EMBASE and EBSCO AHL searches were combined with the trial filters eloped by the Scottish Intercollegiate Guidelines Net- rk (SIGN) (Scottish Intercollegiate Guidelines Network, 9). The full electronic search strategy used in The hrane Central Register of Controlled Trials (CENTRAL) is sented in Box 1. Prior to conducting the electronic searches, experts re contacted to enquire about ongoing and recently lished trials in the area of wound care. Citations within ained reviews and relevant papers were scrutinised to ntify additional trials. Study selection: The titles and abstracts of the search ults were independently assessed for eligibility and vance by two authors and the full copies of all entially relevant trials were obtained. Decisions on l inclusion after full text assessment was made by one hor and checked by a second; disagreements were resolved by discussion with a third author. Rejected trials were checked by a third author. Data collection process (including data items): Details of
- 14. eligible trials were extracted by two review authors independently and summarised using a data extraction sheet. Disagreements were resolved by discussion with a third author. Data extracted from each study included patient characteristics, care setting, key baseline variables (age, sex, baseline risk, baseline area of existing ulcers), description of the interventions, number of patients randomised to each intervention, description of any co- interventions/standard care, follow-up period, outcomes and acceptability/reliability of equipment if reported. If data were missing from reports, attempts were made to contact the study author to complete the information necessary for the analysis and risk of bias assessment. If trials were published more than once, they were maxi- mally data extracted and a primary reference cited. Risk of bias in individual trials: The methodological and reporting quality of each trial was assessed by a single author and checked by a second using a risk of bias assessment tool which addressed the fulfilment criteria as ‘low risk of bias’, ‘high risk of bias’ or ‘unsure’ (Higgins et al., 2009). This involved examining whether there was evidence of true randomisation; allocation concealment; baseline comparability of groups; blinded outcome assessment and intention-to-treat analysis. Eligible trials were also assessed for incomplete outcome data; drop-out rates and whether the study was free of selective outcome reporting. Dis- agreements were resolved by discussion with a third author. Summary measures (including synthesis of results): Analysis was conducted using RevMan software (Review Manager (RevMan) Version 5.0, 2008). If appropriate data were available from included trials, dichotomous variables of new pressure ulcers developed are presented as risk ratio (RR) with 95% confidence intervals (CIs). When continuous outcome variables, such as change in pressure
- 15. ulcer size or time of pressure ulcer development, were measured, they were summarised using the mean difference (MD). Where possible, Grade 1 pressure ulcers (that is, those which resulted in non-blanchable redness of the skin) were separated from Grade 2 or higher pressure ulcers (Grade 2 generally refers to partial thickness loss of dermis and higher Grades 3 and 4, respectively, refer to full thickness tissue loss and full thickness tissue loss with exposed bone, tendon or muscle (EPUAP-NPUAP 2009)) in order to report on important clinical outcomes. Of the trials that included people with pre-existing pressure ulcers, only the incidence of new pressure ulcers was reported. Trials with similar patients, comparisons and outcomes were considered for pooled analysis. When there was more than one trial comparing similar devices using the same outcome measure (though possibly differing lengths of follow up), statistical heterogeneity was assessed using I2 and tested for by chi-squared test. A value of I2 greater than 50% indicated substantial heterogeneity and was consid- ered significant where p < 0.10 (Higgins et al., 2003). In the absence of significant statistical heterogeneity, trials with similar comparisons were pooled using a fixed effect model (Higgins et al., 2011). Where there was substantial statistical heterogeneity we pooled the data using the ox 1. Search strategy used in The Cochrane Central egister of Controlled Trials (CENTRAL). 1 MeSH descriptor Beds explode all trees 2 mattress* 3 cushion*
- 16. 4 ‘‘foam’’ or transfoam 5 overlay* 6 ‘‘pad’’ or ‘‘pads’’ 7 ‘‘gel’’ 8 pressure NEXT relie* 9 pressure NEXT reduc* 10 pressure NEXT alleviat* 11 ‘‘low pressure’’ NEAR/2 device* 12 ‘‘low pressure’’ NEAR/2 support 13 constant NEAR/2 pressure 14 ‘‘static air’’ 15 alternat* NEXT pressure 16 air NEXT suspension* 17 air NEXT bag* 18 water NEXT suspension* 19 elevation NEAR/2 device* 20 clinifloat or maxifloat or vaperm or therarest or sheepskin or hammock or ‘‘foot waffle’’ or silicore
- 17. or Pegasus or cairwave 21 (turn* or tilt*) NEXT (bed* or frame*) 22 kinetic NEXT (therapy or table*) 23 net NEXT bed* 24 ‘‘positioning’’ or ‘‘repositioning’’ 25 (#1 OR #2 OR #3 OR #4 OR #5 OR #6 OR #7 OR #8 OR #9 OR #10 OR #11 OR #12 OR #13 OR #14 OR #15 OR #16 OR #17 OR #18 OR #19 OR #20 OR #21 OR #22 OR #23 OR #24) 26 MeSH descriptor Pressure Ulcer explode all trees 27 pressure NEXT (ulcer* or sore*) 28 decubitus NEXT (ulcer or sore*) 29 (bed NEXT sore*) or bedsore* 30 (#26 OR #27 OR #28 OR #29) 31 (#25 AND #30) E. McInnes et al. / International Journal of Nursing Studies 49 (2012) 345–359348 random-effects model (Higgins et al., 2011). For the purpose of meta-analysis it was assumed that risk ratio
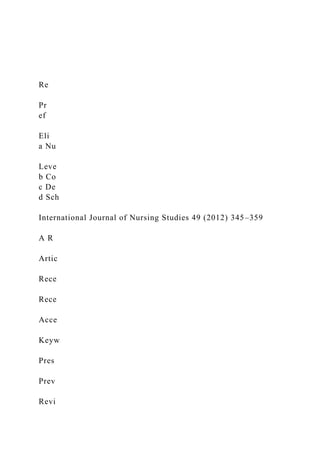
- 18. remained constant for different lengths of follow up, hence we pooled trials which followed participants for different lengths of time. Where pooling was inappropriate, the results of the trials were reported narratively. 3. Results Fifty-three eligible randomised trials were identified with a total of 16,285 study participants. Fig. 1 shows the study selection process. Of the 112 full-text articles assessed for eligibility, 59 were excluded for a variety of reasons as detailed in Fig. 1. The trials were conducted in a variety of settings including operating theatres, intensive care units, ortho- paedic hospital units, accident and emergency units, extended care facilities and nursing homes. Sample sizes ranged from 12 to 1972 participants and the reported follow-up periods for trials ranged from one day to 12 months. Similar timing of outcome assessment between groups under investigation was reported in 34 trials and these ranged from daily to weekly. The methodological quality of the included trials is presented in Table 1. Use of a randomly generated allocation sequence was evident in 24 trials (Bennett et al., 1998; Cadue et al., 2008; Cooper et al., 1998; Economides et al., 1995; Gentilello et al., 1988; Geyer et al., 2001; Gilcreast et al., 2005; Kemp et al., 1993; Keogh and Dealey, 2001; Lazzara and Buschmann, 1991; McGowan et al., 2000; Mistiaen et al., 2009; Nixon et al., 2006, 1998; Price et al., 1999; Russell and Lichtenstein, 2000; Russell et al., 2003; Sanada et al., 2003; Santy et al., 1994; Schultz et al., 1999; Summer et al., 1989; Tymec et al., 1997; Vanderwee et al., 2005; Vyhlidal et al., 1997). Methods of randomisation used
- 19. included table of random numbers, automated phone systems and computerised random number generators. Adequate allocation concealment – defined as those involved in enrolling participants not being able to foresee allocation through the use of central allocation, including telephone or web-based randomisation, or sequentially numbered, opaque, sealed envelopes – was evident in 16 Recor ds identified throu gh database searching (n = 184) Sc re en in g In cl ud ed E lig ib ili ty
- 20. Id en ti fi ca ti on Additional records ide ntifie d through other sources (n = 11) Records afte r duplicates re mov ed (n =19 5 ) Recor ds screened (n = 19 5) Reco rds ex clud ed (n = 83) Full-te xt article s as sessed for eligibility (n = 112) Full-text articles excluded, wit h reason s (n = 59) Literatur e revi ews (n=2)
- 21. Incomple te data (n=8) Did not report clinical outcome (n=20) Not a trial (n=11) Different intervention (n=9) Other inc lusion criteria not met (n=9 ) Total trials in review (n = 53) Fig. 1. PRISMA flow diagram of study selection. tria 199 199 et a Tay Wh rep et a Gra Tab Risk St An Ar Be
- 24. Ru Sa Sa Sc Sid St Su Ta Ta Th Ty Va Vy W E. McInnes et al. / International Journal of Nursing Studies 49 (2012) 345–359 349 ls (Cadue et al., 2008; Cobb et al., 1997; Cooper et al., 8; Economides et al., 1995; Geyer et al., 2001; Gray et al., 8; Jolley et al., 2004; Keogh and Dealey, 2001; Mistiaen l., 2009; Nixon et al., 2006, 1998; Sanada et al., 2003; lor, 1999; Theaker et al., 2005; Vanderwee et al., 2005; itney et al., 1984). Blinding of outcome assessment was
- 25. orted in 10 trials (Cavicchioli and Carella, 2007; Conine l., 1990, 1994; Feuchtinger et al., 2006; Geyer et al., 2001; y et al., 1998; Nixon et al., 1998; Russell et al., 2000; Schultz, 1998; Theaker et al., 2005). Twenty-five trials adequately addressed incomplete outcome data, for exam- ple, by either having balanced or no missing outcome data, or having missing data that have been imputed using appropriate methods (Aronovitch et al., 1999; Bennett et al., 1998; Cadue et al., 2008; Cavicchioli and Carella, 2007; Cobb et al., 1997; Conine et al., 1990, 1993, 1994; Cooper et al., 1998; Gebhardt et al., 1996; Geyer et al., 2001; Gilcreast et al., 2005; Laurent, 1997; Lim et al., 1988; McGowan et al., le 1 of bias of included trials. udy Adequate sequence generation Allocation concealment Blinding Incomplete outcome data addressed Free of
- 26. selective reporting Groups similar at baseline Timing of outcome assessment similar in all groups dersen et al. (1982) Unclear Unclear Unclear Unclear Low risk Low risk Low risk onovitch et al. (1999) Unclear Unclear Unclear Low risk Low risk Low risk Low risk nnett et al. (1998) Low risk Unclear Unclear Low risk High risk Low risk High risk due et al. (2008) Low risk Low risk Unclear Low risk Unclear Low risk Low risk vicchioli and Carella (2007) Unclear Unclear Low risk Low risk Low risk High risk Low risk bb et al. (1997) Unclear Low risk Unclear Low risk Low risk
- 27. High risk High risk llier (1996) Unclear Unclear High risk Unclear Low risk Unclear High risk nine et al. (1990) Unclear Unclear Low risk Low risk Unclear Low risk Unclear nine et al. (1993) Unclear Unclear Unclear Low risk Low risk Low risk Low risk nine et al. (1994) Unclear Unclear Low risk Low risk Low risk Low risk Low risk oper et al. (1998) Low risk Low risk Unclear Low risk Low risk Low risk Low risk echsel and Conine (1985) Unclear Unclear Unclear Unclear Low risk Low risk Low risk onomides et al. (1995) Low risk Low risk Unclear Unclear Low risk Low risk Low risk ing et al. (1964) Unclear Unclear Unclear Unclear Low risk Unclear Low risk ton-Smith et al. (1982) High risk Unclear Unclear Unclear High risk Low risk High risk uchtinger et al. (2006) Unclear Unclear Low risk Unclear Low risk Low risk Low risk bhardt et al. (1996) Unclear Unclear Unclear Low risk Unclear Low risk Unclear ntilello et al. (1988) Low risk Unclear Unclear Unclear Unclear
- 28. Low risk High risk yer et al. (2001) Low risk Low risk Low risk Low risk Low risk Low risk Low risk lcreast et al. (2005) Low risk High risk High risk Low risk Unclear Unclear Low risk ldstone et al. (1982) Unclear Unclear Unclear High risk Low risk Low risk Low risk ay and Campbell (1994) Unclear Unclear Unclear Unclear Unclear Unclear High risk ay et al. (1998) Unclear Low risk Low risk Unclear Unclear Unclear Low risk nningberg et al. (2000) Unclear Unclear Unclear Unclear High risk Low risk Unclear mpton (1997) Unclear Unclear Unclear Unclear Unclear Unclear Unclear fman et al. (1994) Unclear Unclear High risk Unclear High risk Low risk Low risk man et al. (1993) Unclear Unclear Unclear High risk High risk Low risk Low risk lley et al. (2004) Unclear Low risk High risk High risk High risk Unclear Low risk mp et al. (1993) Low risk Unclear Unclear High risk High risk Unclear Low risk ogh and Dealey (2001) Low risk Low risk Unclear High risk
- 29. High risk Low risk Low risk urent (1997) Unclear Unclear High risk Low risk Low risk Low risk Low risk zzara and Buschmann (1991) Low risk Unclear Unclear Unclear Low risk Low risk Low risk et al. (1988) Unclear Unclear Unclear Low risk Low risk Low risk Low risk cGowan et al. (2000) Low risk Unclear High risk Low risk Low risk Low risk Low risk istiaen et al. (2009) Low risk Low risk High risk Unclear Unclear Low risk Low risk xon et al. (1998) Low risk Low risk Low risk Low risk Low risk High risk Low risk xon et al. (2006) Low risk Low risk High risk Low risk Low risk Low risk Low risk ice et al. (1999) Low risk Unclear High risk Unclear Low risk Low risk Low risk ssell et al. (2000) Low risk Unclear Low risk Low risk Low risk Low risk Low risk ssell et al. (2003) Low risk Unclear High risk Low risk Low risk Low risk Low risk nada et al. (2003) Low risk Low risk Unclear High risk Low risk Low risk Low risk nty et al. (1994) Low risk Unclear Unclear Unclear Low risk
- 30. Low risk Low risk hultz et al. (1999) Low risk High risk Low risk Low risk Low risk Low risk Low risk eranko et al. (1992) Unclear Unclear Unclear Unclear Low risk Unclear Unclear apleton (1986) Unclear Unclear Unclear Low risk Unclear Low risk Unclear mmer et al. (1989) Low risk Unclear Unclear Low risk Low risk Unclear Unclear kala et al. (1996) Unclear High risk Unclear Low risk Low risk Low risk Unclear ylor (1999) Unclear Low risk Unclear Unclear High risk Low risk Unclear eaker et al. (2005) Unclear Low risk Low risk Unclear Low risk Low risk Unclear mec et al. (1997) Low risk Unclear Unclear Unclear Low risk Unclear Unclear nderwee et al. (2005) Low risk Low risk Unclear Unclear Unclear Low risk Unclear hlidal et al. (1997) Low risk Unclear Unclear Low risk Low risk High risk Unclear hitney et al. (1984) Unclear Low risk Unclear Low risk Low risk Unclear Low risk
- 31. E. McInnes et al. / International Journal of Nursing Studies 49 (2012) 345–359350 2000; Nixon et al., 2006, 1998; Russell and Lichtenstein, 2000; Russell et al., 2003; Schultz et al., 1999; Stapleton, 1986; Summer et al., 1989; Takala et al., 1996; Vyhlidal et al., 1997; Whitney et al., 1984). Thirty-three trials were judged to be free of selective outcome reporting (Andersen et al., 1982; Aronovitch et al., 1999; Cavicchioli and Carella, 2007; Cobb et al., 1997; Collier, 1996; Conine et al., 1993, 1994; Cooper et al., 1998; Daechsel and Conine, 1985; Economides et al., 1995; Ewing et al., 1964; Feuchtinger et al., 2006; Geyer et al., 2001; Goldstone et al., 1982; Laurent, 1997; Lazzara and Buschmann, 1991; Lim et al., 1988; McGowan et al., 2000; Nixon et al., 2006, 1998; Price et al., 1999; Russell and Lichtenstein, 2000; Russell et al., 2003; Sanada et al., 2003; Santy et al., 1994; Schultz et al., 1999; Sideranko et al., 1992; Summer et al., 1989; Takala et al., 1996; Taylor, 1999; Theaker et al., 2005; Tymec et al., 1997; Vyhlidal et al., 1997; Whitney et al., 1984). Thirty-seven trials reported that participant groups under investigation were similar regard- ing prognostic factors (including age, sex, continence and/or reasons for immobility) (Andersen et al., 1982; Aronovitch et al., 1999; Bennett et al., 1998; Cadue et al., 2008; Conine et al., 1990, 1993, 1994; Cooper et al., 1998; Daechsel and Conine, 1985; Economides et al., 1995; Exton-Smith et al., 1982; Feuchtinger et al., 2006; Gebhardt et al., 1996; Gentilello et al., 1988; Geyer et al., 2001; Goldstone et al., 1982; Gunningberg et al., 2000; Hofman et al., 1994; Inman et al., 1993; Keogh and Dealey, 2001; Laurent, 1997; Lazzara and Buschmann, 1991; Lim et al., 1988; McGowan et al., 2000; Mistiaen et al., 2009; Nixon et al., 2006; Price et al., 1999; Russell and Lichtenstein, 2000; Russell et al., 2003; Sanada et al., 2003; Santy et al., 1994; Schultz et al., 1999; Stapleton, 1986; Takala et al., 1996; Taylor, 1999; Theaker et al., 2005; Vanderwee et al., 2005).
- 32. Thirteen trials included patients with pre-existing pressure ulcers. Of these, seven included only those with Grade 1 pressure ulcers (Cavicchioli and Carella, 2007; Exton-Smith et al., 1982; Hofman et al., 1994; Keogh and Dealey, 2001; Mistiaen et al., 2009; Nixon et al., 1998; Vanderwee et al., 2005), three included Grades 1 and 2 (Bennett et al., 1998; Nixon et al., 2006; Santy et al., 1994), and one study included only those that were Grade 4 (Economides et al., 1995). For two trials it was not clear what grades of pressure ulcer were included (Feuchtinger et al., 2006; Lazzara and Buschmann, 1991) and for 14 trials it was unclear or unstated whether pre-existing pressure ulcers were included. Trials were classified into those that evaluated ‘low- tech’ devices, ‘high-tech’ devices and other types of support surfaces. This classification system is commonly used, for example in national clinical guidelines (National Institute for Clinical Excellence, 2003). Twenty-three trials evaluated low-tech constant low- pressure support surfaces (foam body supports, sheep- skin overlay, heel devices and mattresses). Twenty-one trials evaluated high tech support surfaces (alternating pressure redistribution devices, low-air-loss beds and air fluidised beds). Other support surfaces included kinetic turning tables (two trials), profiling beds (one study), operating table overlays (six trials) and seat cushions (four trials). Characteristics of the included Tables 1 and 2, respectively. Table 3 shows the results of analyses. 4. Comparisons: ‘low-tech’ constant low pressure support surfaces
- 33. 4.1. Comparisons between ‘low-tech’ constant low pressure support surfaces and standard foam surfaces Nine trials evaluated a standard foam hospital mat- tress compared with a ‘low-tech’ constant low pressure support surface, including: water-filled mattresses (Andersen et al., 1982); alternative foam mattresses (Collier, 1996; Gray and Campbell, 1994; Hofman et al., 1994; Russell et al., 2003; Santy et al., 1994); bead beds (Goldstone et al., 1982); visco-elastic mattresses (Gun- ningberg et al., 2000) and other low-tech mattresses (Takala et al., 1996). The five trials (Collier, 1996; Gray and Campbell, 1994; Hofman et al., 1994; Russell et al., 2003; Santy et al., 1994) comparing foam alternatives with the standard hospital mattress were pooled using a random effects model (I2 = 77%, x2 13.24, df = 3, p = 0.004). This analysis yielded a pooled risk ratio of 0.40 (95% CI 0.21–0.74) or a relative reduction of pressure ulcer incidence of 60% (95% CI 26– 79%), favouring the use of the foam alternative support surfaces. The high heterogeneity in standard hospital mattresses amongst these trials led to a separate meta- analysis of four UK-based trials (Collier, 1996; Gray and Campbell, 1994; Russell et al., 2003; Santy et al., 1994) as variation in the standard hospital mattress is likely to be lower in the UK. This analysis showed a significant benefit of alternative foam over standard foam being maintained (RR 0.41, 95% CI 0.19–0.87). As heterogeneity in this pooled group was high (I2 = 84%, x2 12.41, df = 2, p = 0.002), Russell et al. (2003) was removed as it was an outlier. Hetero- geneity was reduced (I2 = 39%) and the pooled results maintained a significant effect in favour of the alternative foam support over the standard support surface (RR 0.29, 95% CI 0.16–0.52).
- 34. The four remaining trials in this category evaluated a range of products against the standard hospital mattresses. The incidence and severity of pressure ulcers in patients deemed at ‘high risk’ were reduced when patients were placed on either a bead filled mattress (Goldstone et al., 1982) (RR 0.32, 95% CI 0.14–0.76), a water-filled mattress (Andersen et al., 1982) (RR 0.35, 95% CI 0.15–0.79) or a constant low-pressure mattress (Takala et al., 1996) (RR 0.06, 95% 0–0.99). Gunningberg et al. (2000) did not find any significant difference in pressure ulcer incidence for those allocated to a visco-elastic foam trolley mattress (in ED) and standard mattress (on the ward) (4/48, 8%) compared with those assigned to a standard trolley mattress (in ED) and standard mattress (on the ward) (8/53, 15%) (p = 0.36). 4.2. Comparisons between alternative foam support surfaces Three trials (Gray et al., 1998; Kemp et al., 1993; Vyhlidal et al., 1997) compared different foam alternatives trials and risk of bias assessment of the trials appear in Table 2 Reported follow-up alternating air
- 35. ess (n = 155) 10 days col (n = 35) vs. 30 days 8) Unclear otation mattress 7 days 18) 6 months 6) vs. foot waffle Unclear (n = 50) 10 days s (n = 50) 10 days upports (43) Unclear isco-elastic foam ttress (A&E) and 14 days or until discharge rd mattress 14 days . standard care Mean: 7 days (experimental group), 7.9 days
- 36. (control group) lid foam overlay 1 month ss (n = 33) 6 months eepskin overlay, tandard hospital devices as Until discharge or transfer = 272) Unclear attress and and cushion Median: 8–14 days (experimental group), 9–17 days (control group) (n = 441) vs. NHS 14 days air mattress Mean: 9.4 days E .
- 39. 3 5 1 Characteristics of included trials. Study (year) Participants Grade 1 pressure ulcers included Intervention (sample size) ‘Low tech’ constant low pressure support surfaces (n = 23)a Andersen et al. (1982)b Patients from the acute setting at high risk of pressure ulcer development (Anderson Scale) No Standard hospital mattress (n = 161) vs. mattress (n = 166) vs. water filled mattr Cadue et al. (2008) Patients from ICU, aged > 18 years. Waterlow score > 10 Nod Foam body support with standard proto Standard protocol (n = 35) Collier (1996) Patients from a general medical ward No Comparison of 8 foam mattresses (n = 7
- 40. Cooper et al. (1998) Patients aged > 65 years from mixed emergency and orthopaedic trauma wards Nod Dry flotation mattress (n = 49) vs. dry fl (n = 51) Ewing et al. (1964) Elderly patients confined to bed, with reduced mobility as a result of neurological disorders, fixed joints or peripheral vascular disease Unclear Sheepskin (n = 18) vs. No sheepskin (n = Gilcreast et al. (2005) Participants from military tertiary academic medical centres, moderate-high risk of pressure ulcer development No Heel protector (n = 77) vs. egg crate (n = 8 (n = 76) Gray and Campbell (1994) Patients from orthopaedic trauma, vascular and medical oncology units, with no breaks in the skin. Waterlow score > 15
- 41. Nod Mattress (n = 50) vs. standard mattress Gray et al. (1998) Patients admitted to a district general hospital, weight < 160 kg Nod Foam mattress (n = 50) vs. foam mattres Goldstone et al. (1982) Patients aged > 60 years with a femur fracture Unclear Bead bed system (n = 32) vs. standard s Gunningberg et al. (2000) c Patients aged > 65 years with a suspected hip fracture, admitted via A&E Nod Visco-elastic foam mattress (A&E) and v overlay (ward) (n = 48) vs. standard ma standard overlay (ward) (n = 53) Hofman et al. (1994) Patients with a fractures neck of femur. Dutch consensus risk scale score > 8 Yes Cubed foam mattress (n = 21) vs. standa (n = 23) Jolley et al. (2004) Patients aged > 18 years, low – moderate risk of developing a pressure ulcer
- 42. No Sheepskin mattress overlay (n = 270) vs (n = 269) Kemp et al. (1993) Patients aged > 65 from general medical, acute geriatric, long-term care wards. Braden score > 16 Nod Convoluted foam overlay (n = 45) vs. so (39) Lazzara and Buschmann (1991) Nursing home residents at risk of pressure ulcer development. Norton score > 15 Unclear Air-filled overlay (n = 33) vs. gel mattre McGowan et al. (2000) Patients aged > 60 years from an extended care facility, at risk of developing a pressure ulcer, use of a wheelchair � 3 h a day. Norton score � 14 Nod Standard hospital mattress and sheets, sh heel and elbow protectors (n = 155) vs. s mattress and sheets and other low-tech required (n = 142)
- 43. Mistiaen et al. (2009) Patients from an aged care facility and rehabilitation centre Yes Sheepskin (n = 271) vs. standard care (n Russell et al. (2003) Patients from acute elderly, orthopaedic and rehabilitation units, aged > 60 years Unclear Visco-polymer energy absorbing foam m cushion (n = 562) vs. standard mattress (n = 604) Santy et al. (1994) Patients aged > 55 years with a hip fracture or pressure ulcers Yes Comparison between 4 foam mattresses standard mattress (n = 64) Sideranko et al. (1992) b Patients from ICU > 48 h Nod Alternating air overlay (n = 20) vs. Static (n = 20) vs. Water mattress (n = 17) Reported
- 44. follow-up olyether foam pad 34) Unclear = 21) vs. standard 14 days pillow (n = unclear) Unclear ss replacement Range: 10 – 21 days r – SSI/Hillrom] Range: 1–60 days w-pressure setting tinuous low- – Hill Rom] 2 weeks 2) vs. Static air = 61) 40 days s. Silicore fibre 3 months
- 45. ) vs. Silicore fibre 3 months uidised bed (n = 6) 2 weeks ) vs. large cell ripple 2 weeks ys/mattresses/beds) pports (overlays/ Unclear vs. Alternating 20 days (maximum) d ICU bed (n = 49) Mean: 17 days ) vs. Alternating 60 days mattress (post-op) ress (ICU) and s. standard mattress attress (post-op) tress (ICU) and ost-op) (n = 77) Unclear = 40) vs. alternating
- 46. 0) 14 days . Single layer air cell mattress (n = 35) Unclear ressure ernative alternating ributing cushion Until discharge lternating pressure 2 weeks post-ICU discharge E . M cIn n e s e t a
- 48. ie s 4 9 (2 0 1 2 ) 3 4 5 – 3 5 9 3 5 2 Table 2 (Continued ) Study (year) Participants Grade 1 pressure ulcers included Intervention (sample size)
- 49. Stapleton (1986) b Female elderly patients with a fractured neck of femur. Norton score < 14. Nod Large cell ripple overlay (n = 32) vs. p (n = 34) vs. Silicore fibre overlay (n = Takala et al. (1996) Patients from ICU with an expected length of stay > 5 days Unclear Continuous low-pressure mattress (n hospital foam mattress (n = 19) Tymec et al. (1997) Patients from large hospital. Braden score < 16 Nod Foot waffle (n = unclear) vs. hospital Vyhlidal et al. (1997) Newly admitted patients to a skilled nursing facility with an estimated stay � 10 days. Braden score < 18 Nod Foam overlay (n = 20) vs. fibre mattre (n = 20) ‘High tech’ pressure support surfaces (n = 18)a Bennett et al. (1998) Acute and long term incontinent patients. In bed > 16 h a day Yes Low-air-loss hydrotherapy [Clensicai (n = 42) vs. standard care (n = 56)
- 50. Cavicchioli and Carella (2007) Acute and long-term care patients at risk of pressure ulcers and an expected admission � 2 weeks. Braden score < 17 or mobility or subscales < 3 respectively Yes High-tech mattress on alternating lo (n = 86) vs. high-tech mattress on con pressure setting (n = 84) [both due 2 Cobb et al. (1997) Patients aged > 18 years from hospital wards and ICU. Expected length of stay 1–2 weeks. Nod Low-air-loss bed [KinAir – KCI] (n = 6 mattress overlay [Waffle – EHOB] (n Conine et al. (1990) Patients aged 18–55 years with evidence of chronic neurological disease Nod Alternating pressure overlay(n = 72) v overlay (n = 76) Daechsel and Conine (1985) Patients from a long-term care hospital with chronic neurological conditions and considered at high risk of
- 51. pressure ulcers Nod Alternating pressure mattress (n = 16 overlay (n = 16) Economides et al. (1995) Patients with stage 4 pressure ulcers requiring myocutaneous flap closure No Dry flotation mattress (n = 6) vs. air-fl Exton-Smith et al. (1982) Newly admitted geriatric patients with a fractured neck of femur Yes Alternating pressure mattress (n = 31 mattress (n = 31) Gebhardt et al. (1996) ICU patients with an admission > 3 days. Norton score < 1 Nod Alternating pressure supports (overla (n = 23) vs. constant low pressure su mattresses/beds) (n = 20) Hampton (1997) No details provided Unclear Alternating pressure mattress (n-36) pressure mattress (n = 39) Inman et al. (1993) Patients aged > 17 years, APACHE score > 15. ICU
- 52. stay > 3 days Unclear Low-air-loss beds (n = 49) vs. standar Nixon et al. (2006) Patients aged > 55 years with an expected length of hospital stay � 7 days. Braden score = 1–2 Yes Alternating pressure overlay (n = 990 pressure mattress (n = 982) Laurent (1997) Patients aged > 15 years and admitted for major cardiovascular surgery. Hospital stay � 5 days with an ICU admission Unclear Standard mattress (ICU) and standard (n = 80) vs. Alternating pressure matt standard mattress (post-op) (n = 80) v (ICU) vs. Continuous low-pressure m (n = 75) vs. Alternating-pressure mat continuous low-pressure mattress (p Price et al. (1999) Patients aged > 60 years with a fractured neck of femur. Medley score > 25 Unclear Low pressure mattress and cushion (n
- 53. pressure mattress and cushion (n = 4 Sanada et al. (2003) Patients from an acute care unit. Bed bound and requiring head elevations. Braden score � 16. Nod Double layer air cell overlay (n = 37) vs overlay (n = 36) vs. standard hospital Taylor (1999) Patients aged > 16 years Nod Alternating pressure mattress with p redistributing cushion (n = 22) vs. alt pressure system with pressure redist (n = 22) Theaker et al. (2005) Patients aged > 80 years from ICU. At high risk of pressure ulcer development Nod Alternating pressure bed (n = 30) vs. a mattress (n = 32) Vanderwee et al. (2005) Patients aged > 18 years from surgical, internal medicine Yes Alternating pressure mattress with air cushion for sitting and air cushion
- 54. Unclear convoluted foam 8 days e] (n = 112) vs. 7 days m cushion 3 months = 73) 3 months ing mattress and (n = 85) vs. ng mattress 5 days entional bed Unclear tandard foam 12 months (n = 50) Range: 5 – 10 days d foam cushion 5 months ard mattress 8 days Conventional 7 days vs. usual care 6 days ntional bed with Unclear
- 57. 5 9 3 5 3 or geriatric hospital wards. An expected hospital stay of � 3 days. Braden score < 17. (n = 222) vs. visco-elastic foam mattress for sitting (n = 225) Whitney et al. (1984) Patients from medical-surgical wards in bed for � 20 h a day Unclear Alternating pressure mattress (n-25) vs. bed (n = 26) ‘Other’ pressure support surfaces (n = 12)a Aronovitch et al. (1999) Patients aged > 18 years, undergoing surgery (>3 h) under general anaesthesia Nod Alternating pressure system [MicroPuls conventional management (n = 105) Conine et al. (1993) Patients aged > 60 years from an extended
- 58. care facility and high risk of a pressure ulcer. Sitting in a wheelchair for � 4 h/day No Slab cushion (n = 144) vs. contoured foa (n = 144) Conine et al. (1994) Elderly patients in an extended care hospital and at high risk of pressure ulcers. Sitting in a wheelchair for � 4 h/ day. Norton score < 14. Unclear Gel cushion (n = 68) vs. foam cushion (n Feuchtinger et al. (2006) Patients aged > 18 years, scheduled for cardiac surgery with extracorporeal circulation Unclear Operating table with water filled warm thermoactive visco elastic foam overlay operating table with water filled warmi (n = 90) Gentilello et al. (1988) Critically ill patients in a surgical ICU, immobilised due to head injury, spinal injuries or traction
- 59. Unclear Kinetic treatment table (n = 27) vs. conv (n = 38) Geyer et al. (2001) Patients aged > 65 years, in a wheelchair. Tolerance of sitting in a wheelchair � 6 h, weight > 250 lbs. Braden score � 18 No Pressure reducing cushion (n = 15) vs. s cushion (n = 17) Keogh and Dealey (2001) Patients aged > 18 years, from surgical and medical wards. Waterlow score = 15–25 Yes Profiling bed (n = 50) vs. flat-based bed Lim et al. (1988) Patients aged > 60 years from an extended care facility. Use of a wheelchair � 3 h/day. Norton score � 14 No Foam slab cushion (n = 26) vs. contoure (n = 26) Nixon et al. (1998) Patients aged > 55 years, admitted for major general, gynaecological or vascular surgery in supine or lithotomy position
- 60. Yes Dry visco elastic pad (n = 222) vs. stand (n = 224) Russell et al. (2000) Patients aged > 18 years, undergoing scheduled cardiothoracic surgery under general anaesthesia and � long Nod Alternating pressure overlay (n = 98) vs. care (n = 100) Schultz et al. (1999) Patients aged > 18 years, admitted for surgery � 2 h in lithotomy position Nod Experimental mattress overlay (n = 206) (n = 207) Summer et al. (1989) Patients from ICU with sepsis, pneumonia, respiratory failure, drug overdose, metabolic coma, stroke, neuromuscular disease or ARDS Unclear Kinetic treatment table (n = 43) vs. conve 2-hourly turning (n = 43) a Does not include trials appearing under another subheading. b Paper is also considered under ‘low-tech constant low
- 61. pressure support surfaces’. c Paper is also considered under ‘other pressure support surfaces’. d Existing pressure ulcers part of exclusion criteria. Table 3 Results of analyses – pressure ulcer incidence. Comparison Number of trials (authors) Participants Risk ratio (95% CI) p-Value* ‘Low tech’ constant low pressure support surfaces Comparison between low-tech CLP and SFM supports Bead bed system vs. Standard supports 1 (Goldstone et al.) 75 0.32 (0.14, 0.76) – Water filled mattress vs. Standard hospital mattress 1 (Andersen et al.) 316 0.35 (0.15, 0.79) – Constant low pressure mattress vs. Standard support 1 (Takala et al.) 40 0.06 (0 to 0.99) – Pooled trials Foam alternatives vs. Standard hospital mattress 5 (Collier, Gray 94, Hofman, Russell 03, Santy) 2016 0.40 (0.21, 0.74) p = 0.004
- 62. Foam alternatives vs. Standard hospital mattress (UK trials only) 4 (Collier, Gray 94, Russell 03, Santy) 1980 0.41 (0.19, 0.87) p = 0.020 Foam alternatives vs. Standard hospital mattress (Russell et al., 2002 excluded) 3 (Collier. Gray 94. Santy) 814 0.29 (0.16, 0.52) p < 0.0001 Comparisons between AFM supports Standard mattress vs. 4 foam mattresses 1 (Santy et al.) 505 0.36 (0.22, 0.59) – Fibre mattress replace vs. foam overlay 1 (Vyhlidal et al.) 40 0.42 (0.18, 0.96) – Convoluted foam overlay vs. Solid foam overlay 1 (Kemp et al.) 84 0.66 (0.37, 1.16) – Foam body support (+standard protocol) vs. Standard protocol 1 (Cadue et al.) 70 0.16 (0.05, 0.49) – Comparison between dry flotation mattresses 1 (Cooper et al.) 84 0.63 (0.16, 2.47) –
- 63. Air filled overlay vs. Gel mattress 1 (Lazzara) 66 0.80 (0.24, 2.72) – Pooled trials: Comparison between sheepskins (all pressure ulcer grades) 3 (Jolley, McGowan, Mistaein) 1281 0.48 (0.31, 0.74) p = 0.0008 Comparison between sheepskins (pressure ulcers Grade 2 and above) 3 (Jolley, McGowan, Mistaein) 1281 Fixed effect: p = 0.04 0.56 (0.32, 0.97) Random effect: p = 0.09 0.60 (0.34, 1.08) ‘High tech’ pressure support surfaces AP: Comparison between AP and SFM supports Pooled trials: Alternating air-mattress vs. Overlay 2 (Andersen, Sanada) 409 0.31 (0.17, 0.58) p = 0.0002 AP: Comparison between AP and CLP supports Pooled trials:
- 64. Silicore vs. foam overlays 4 (Conine 90, Daeschel, Stapleton, Whitney) 31 0.91 (0.72, 1.16) p = 0.46 Alternating pressure device vs. static water/ air mattresses 3 (Andersen, Sideranko, Price) 458 1.31 (0.51, 3.35) p = 0.57 Alternating pressure devices vs. constant low-pressure support 10 (Andersen, Cavicchioli, Conine 90, Daeschel, Gebhardt, Price, Sideranko, Stapleton, Vanderwee, Whitney) 1606 0.85 (0.64, 1.13) p = 0.28 LAL beds Alternating pressure device vs. static water/ air mattresses 1 (Bennett et al.) 98 2.67 (0.86, 8.27) – Pooled trials: Comparison between LAL beds 2 (Inman, Cobb) 221 0.33 (0.16,
- 65. 0.67) p = 0.002 Air-fluidised beds Air fluidised bed vs. dry flotation mattress 1 (Economides et al.) 12 1.00 (0.20, 4.95) – Other pressure supports Kinetic turning tables Pooled trials: Comparison between kinetic turning table and conventional bed 2 (Gentillelo, Summer) 151 1.23 (0.57, 2.65) p = 0.59 Operating table overlays Water filled warming mattress and overlay vs. water filled warming mattress 1 (Feuchtinger et al.) 175 1.53 (0.69, 3.39) – Dry visco-elastic pad vs. standard mattress 1 (Nixon et al., 98) 65 0.53 (0.33, 0.85) – Pooled trials: Alternating pressure system intraoperatively vs. conventional care
- 66. 2 (Aronovitch, Russell 00) 368 0.21 (0.06, 0.70) p = 0.01 Seat cushions Slab cushion vs. contoured foam cushion 1 (Conine et al., 93) 248 1.00 (0.84, 1.18) – E. McInnes et al. / International Journal of Nursing Studies 49 (2012) 345–359354 and eva pre ma (RR pre ing 0.6 com Gra (Gr 4.3. com to s et a wa 4.2 pre she tria
- 68. * E. McInnes et al. / International Journal of Nursing Studies 49 (2012) 345–359 355 are reported as individual results below as the luated interventions are heterogeneous. Vyhlidal et al. (1997) found a significant reduction in ssure ulcer incidence in people randomised to a fibre ttress replacement when compared with a foam overlay 0.42, 95% CI 0.18–0.96). No significant differences in ssure ulcer incidence rates were found when compar- a convoluted foam overlay and a solid foam overlay (RR 6, 95% CI 0.37–1.16) (Kemp et al., 1993) or in parison of two foam mattresses, Transfoam (one de 4 ulcer) and Transfoamwave (one Grade 2 ulcer) ay et al., 1998). Other ‘low-tech’ support surfaces with various parisons Three trials evaluating the use of sheepskins compared tandard care were pooled (Jolley et al., 2004; McGowan l., 2000; Mistiaen et al., 2009). A random effects model s used as heterogeneity was substantial (I2 = 52%, x2 0, df = 2, p = 0.12). There were significantly fewer ssure ulcers of any grade amongst those allocated to epskins (RR 0.48, 95% CI 0.31–0.74). Across the three ls, out of 1281 participants, 51 ulcers were Grade 2 and her (3 participants developed an ulcer of Grades 3 or 4)
- 69. most ulcers were Grade 1. An analysis examining de 2 and higher pressure ulcers yielded significant ults (RR 0.56, 95% CI 0.32–0.97) using a fixed effects lysis as (I2 = 3%, x2 2.06, df = 2, p = 0.36). However, a dom effects analysis was also undertaken due to the thodological heterogeneity (in terms of the participants quality of the trials), and this was not significant (RR 0, 95% CI 0.34–1.08). A significant reduction in pressure ulcer incidence s found in a study comparing a foam body support h a standard care protocol which included a water ttress, half seated position and massages (RR 0.16, CI 0.05–0.49) (Cadue et al., 2008). A comparison of a l support surface (foot waffle) with elevation of heels ng a hospital pillow, reported the incidence of ssure ulcers in the foot waffle group (n = 6) to be le that of the comparison group (n = 2) (study group bers were not specified) (Tymec et al., 1997). ther evaluation of a foot waffle (5/76), egg crate 87) and bunny boot (3/77) showed no differences, ever, it was not clear whether the results related to number of ulcers or the number of people with ers (Gilcreast et al., 2005). Comparisons of two dry flotation mattresses (Cooper l., 1998); a gel mattress and an air filled overlay (Lazzara Buschmann, 1991); alternating air overlay, static air ttress and a water mattress (Sideranko et al., 1992)
- 70. and a large cell ripple mattress, polyether foam bed and a Spenco pad (Stapleton, 1986), found no significant differences. 5. Comparisons: ‘high-tech’ pressure support surfaces 5.1. Comparisons between alternating pressure supports and standard hospital mattress Two trials which compared alternative pressure sup- ports compared with a standard hospital mattress (Andersen et al., 1982; Sanada et al., 2003) were pooled using a fixed effect model (I2 = 0%, x2 0.02, df = 1, p = 0.0002). There was a significant reduction in pressure ulcer development favouring the alternating pressure surface (RR 0.31, 95% CI 0.17–0.58). 5.2. Comparisons between alternating pressure supports and constant low pressure supports No significant differences were found between Silicore or foam overlays and alternating pressure devices when pooling four studies (RR 0.91; 95% CI 0.72–1.16) (Conine et al., 1990; Daechsel and Conine, 1985; Stapleton, 1986; Whitney et al., 1984). Nor were significant differences found in a pooled analysis comparing alternating pressure devices and static water or static air mattresses (Andersen et al., 1982; Price et al., 1999; Sideranko et al., 1992) (RR 1.31, 95% CI 0.51–3.35). A pooled random effects analysis of 10 RCT’s comparing various constant low-pressure devices and alternating- pressure devices (Andersen et al., 1982; Cavicchioli and Carella, 2007; Conine et al., 1990; Daechsel and Conine,
- 71. 1985; Gebhardt et al., 1996; Price et al., 1999; Sideranko et al., 1992; Stapleton, 1986; Vanderwee et al., 2005; Whitney et al., 1984) found no significant difference between the devices (RR 0.85; 95% CI 0.64–1.13). A comparison of various combinations of standard, constant low-pressure and alternating pressure mattresses showed no significant benefits of using alternating pressure in surgical intensive care patients intra- and post-ICU (Laurent, 1997). 5.3. Comparisons between different alternating pressure devices A two-layer large cell ripple alternating pressure device was found to be significantly more effective in preventing pressure ulcers compared with another alternating-pres- sure device (16% vs. 34%, p > 0.05) (Exton-Smith et al., 1982). No other significant differences were observed in any of the other four trials in this group. le 3 (Continued ) mparison Number of trials (authors) Participants Risk ratio (95% CI) p-Value* 1 (Lim et al.) 52 1.06 (0.75, 1.49) – at cushion vs. standard cushion 1 (Geyer et al.) 32 0.68 (0.33, 1.42) – y cushion vs. foam cushion 1 (Conine et al., 94) 141 0.61 (0.37, 1.00) – p-values only reported for pooled analyses.
- 72. E. McInnes et al. / International Journal of Nursing Studies 49 (2012) 345–359356 5.4. Low-air-loss and air-fluidised beds Three trials evaluated the use of low-air-loss beds in preventing pressure ulcers (Bennett et al., 1998; Cobb et al., 1997; Inman et al., 1993). Of these, two that compared low-air-loss beds with a bed and overlay were pooled using random effects (I2 = 26%) (Cobb et al., 1997; Inman et al., 1993). A significant difference in favour of the low-air-loss beds was found (RR 0.33, 95% CI 0.16–0.67). The comparison between low-air-loss hydrotherapy and standard care (Bennett et al., 1998) found that there was a higher pressure ulcer incidence amongst those study participants cared for on a the low-air-loss hydro support surface (19%) compared to those who received standard care (7%) (RR 2.67, 95% CI 0.86–8.27). No significant differences were found between an air-fluidised bed and a dry flotation mattress (Economides et al., 1995). 6. Comparisons between other pressure supports 6.1. Operating table overlays Two trials compared the Micropulse system with a gel pad during surgery and a standard mattress post- operatively (Aronovitch et al., 1999, Russell and Lichten- stein, 2000). These two trials were pooled (fixed effect model I2 = 0%, x2 0.40, df = 1, p = 0.01) and the Micropulse system was found to be significantly better at preventing pressure ulcers (RR 0.21, 95% CI 0.06–0.70). There was a significant reduction in the incidence of
- 73. post-operative pressure ulcers in participants allocated a dry visco-elastic pad compared to standard care (RR 0.53, 95% CI 0.33–0.85) (Nixon et al., 1998). Schultz et al. (1999) reported a higher incidence of pressure ulcers in patients in the overlay group (26.6%) compared with 16.4% in the standard care group (16.4%). More details about this study was sought from the author but were not forthcoming. The study by Feuchtinger et al. (2006) was terminated because more people in the thermoactive viscoelastic foam overlay group developed pressure ulcers (2 compared to one in the group allocated a water-filled warming mattress without the overlay). 6.2. Kinetic turning tables and profiling beds Using a fixed effect model (I2 = 0%, x2 0.35, df = 1, p = 0.59), there was no evidence of a significant difference between kinetic turning tables compared with conven- tional beds (Gentilello et al., 1988, Summer et al., 1989) (RR 1.23, 95% CI 0.57–2.65). Keogh et al. reported that no pressure ulcers occurred in those cared for on a profiling bed or on a flat-based bed. 6.3. Seat cushions Four trials (Conine et al., 1993, 1994; Geyer et al., 2001; Lim et al., 1988) evaluated the use of seat cushions. No significant differences were found in the two trials that compared slab and contoured foam cushions (Conine et al., 1993; Lim et al., 1988) (RR 1.00, 95% CI 0.84–1.18) and (RR 1.06, 95% 0.75–1.49). Nor were differences found between a pressure redistribution seat cushion compared with a standard cushion (Geyer et al., 2001: RR 0.68, 95% CI 0.33– 1.42) or between a Jay cushion and foam cushion (Conine
- 74. et al., 1994: RR 0.61, 95% CI 0.37–1.00). 7. Discussion This systematic review shows that a range of foam- based, low pressure mattresses and overlays, sheepskins, and also some ‘higher-tech’ support surfaces are more effective than either standard hospital mattresses or standard care in preventing pressure ulcers. In terms of operating theatre support surfaces, Nixon et al. (1998) found a gel-filled overlay to be significantly better than a standard operating table. However, in two other trials a gel-filled overlay on the operating table was less effective than an alternating pressure overlay (the Micropulse system) intra- and post-operatively (Aronovitch et al., 1999; Russell and Lichtenstein, 2000). However in these two trials it is not clear whether this is the result of better postoperative pressure relief. Two other trials (Feuchtinger et al., 2006; Schultz et al., 1999) reported post-operative skin changes as a result of different operating theatre overlays. However, the clinical importance of these results is difficult to ascertain in the absence of details from the authors such as pressure ulcer grading and comprehensive descriptions of products evaluated. In addition, it is difficult to separate out the role of postoperative care and concomitant interventions; either of which may have caused the skin changes (mainly found on buttock and coccyx). There are indications that two other interventions may also be harmful. Firstly, Foot Waffle heel elevators were associated with a non-significant trebling in the incidence of pressure ulcers in a small trial (Tymec et al., 1997). In another small trial over double the number of those cared for on a low-air-loss hydro support surface developed pressure ulcers compared to those allocated standard care
- 75. (Bennett et al., 1998). However, neither of these trials provided clear information to indicate that the groups were similar at baseline in relation to the most important prognostic factors. Despite the number of comparisons and different products evaluated there remain gaps in the knowledge base for which a rational research agenda could be developed. For example, air fluidised therapy as a prevention strategy has only been compared with dry flotation, and low-air-loss only with standard care. The results of meta-analyses of trials of sheepskins are sensitive to the outcome measure selected. When analysis is confined to Grade 2 and higher pressure ulcers, any significant reduction in pressure ulcer incidence associated with sheepskin disappears. The results reported in the three studies are based predominantly on Grades 1 and 2 pressure ulcers, so the effects of sheepskins on preventing more severe ulcers is uncertain. The estimates obtained when analysing only Grade 2 and higher pressure ulcers varied whether using a fixed effects (results significant) or random effects (results not significant) model. While there is some evidence that sheepskin reduced overall ulceration incidence, once we sample the evidence using Grade 2 and hig het the act and Gra Fur she Gra
- 77. rev 200 effe et a 8. C and sur How as pre bee are E. McInnes et al. / International Journal of Nursing Studies 49 (2012) 345–359 357 her pressure ulcers, the power is reduced and the erogeneity means that we cannot be fully confident of results. It can be postulated that the likely mode of ion of sheepskin will reduce friction but not pressure therefore would be likely to impact on the incidence of de 2 ulcers but not on more severe pressure damage. ther evaluations are therefore required of medical epskins of sufficient power to identify an effect on de 2 ulcer incidence versus Grade 3 and higher. Strengths and limitations Generally, the risk of bias in the included trials was h. While recent trials have improved reporting of some dy details, common methodological flaws included lack llocation concealment, lack of baseline comparability, h attrition rates, lack of intention to treat analysis, lack
- 78. blind or independently verified outcome assessment. s than half of the trials included sample size estimates small sample size was a limitation in many. Other flaws include failure to report on pressure ulcer us on study entry. In many trials the definitions of ssure ulcer free’, ‘low-risk’, ‘moderate-risk’ and ‘high- ’ varied widely and in some trials we were unable to ertain whether study participants with Grade 1 ulcers re accepted into the sample and included in the lyses. ‘Standard care’ was poorly described in many ls and clear descriptions of interventions were also n lacking. Many of the trials reviewed did not provide rmation about co-interventions, such as repositioning, whether these were provided equally to each study . In terms of publication bias, it is important to note that ny of the published trials identified had received some ding from manufacturers. It is also important for the der to be aware that in the older trials the materials d in the production of support surfaces may no longer used. The strengths of our systematic review are the rigorous rching and sifting methods, double data extraction and ble assessment of risk of bias using a standardised tool that we made attempts to contact study authors to ain additional information when needed. Our findings also consistent with a systematic review of RCT’s and si-randomised trials investigating the prevention of l pressure ulcers (Junkin and Gray, 2009) a systematic iew on general pressure ulcer prevention (Reddy et al.,
- 79. 6) and a review of three trials investigating the ctiveness of Australian Medical Sheepskins (Mistiaen l., 2010). onclusion A range of products such as low pressure mattresses overlays, sheepskins, and some ‘higher-tech’ support faces are effective at preventing pressure ulcers. ever, the relative merits of some interventions such higher-tech constant low pressure and alternating ssure remain unclear. The use of seat cushions has not n adequately evaluated and the findings of some trials trials should address the deficiencies discussed above while adhering to the CONSORT statement and also collect data on aspects of equipment performance such as reliability. Conflict of interest None declared. References Allman, R.M., 1997. Pressure ulcer prevalence, incidence, risk factors, and impact. Clinical Geriatric Medicine 13 (3), 421–436. Andersen, K.E., Jensen, O., Kvorning, S.A., Bach, E., 1982. Decubitus pro- phylaxis: a prospective trial on the efficiency of alternating pressure air mattresses and water mattresses. Acta Dermato- Venereologica
- 80. (Stockholm) 63 (3), 227–230. Aronovitch, S.A., Wilber, M., Slezak, S., Martin, T., Utter, D., 1999. A comparative study of an alternating air mattress for the prevention of pressure ulcers in surgical patients. Ostomy/Wound Management 45 (3) pp. 34–40 42–34. Australian Commission for Safety and Quality in Health Care (ACSQHC), 2005. Adverse Event Rates Fact Sheet. Commonwealth of Australia. Banks, V., 1998. Nutrition and pressure area management. Journal of Wound Care 7 (6), 318–319. Bennett, R.G., Baran, P.J., DeVone, L.V., Bacetti, H., Kristo, B., Tayback, M., et al., 1998. Low airloss hydrotherapy versus standard care for incontinent hospitalized patients. Journal of the American Geriatric Society 46 (5), 569–576. Berlowitz, D.R., Brandeis, G.H., Anderson, J., Brand, H.K., 1997. Predictors of pressure ulcer healing among long-term care residents. Journal of the American Geriatrics Society 45 (1), 30–34. Bianchetti, A., Zanetti, O., Rozzini, R., Trabucchi, M., 1993. Risk factors for the development of pressure sores in hospitalized elderly patients:
- 81. results of a prospective study. Archives of Gerontology and Geriatrics 16 (3), 225–232. Cadue, J.F., Karolewicz, S., Tardy, C., Barrault, C., Robert, R., Pourrat, O., 2008. Prevention of heel pressure sores with a foam body- support device. A randomized controlled trial in a medical intensive care unit. Presse Medicale 37 (1 Suppl. Part 1), 30–36. Casey, G., 1998. The importance of nutrition in wound healing. Nursing Standard 13 (3), 51–52. Casey, G., 1997. Nutrition helps wound healing. Nursing New Zealand 3 (11) 19–19. Cavicchioli, A., Carella, G., 2007. Clinical effectiveness of a low-tech versus high-tech pressure redistributing mattress. Journal of Wound Care 16 (7), 285–289. Cobb, G.A., Yoder, L.H., Warren, J.B., 1997. Pressure Ulcers: Patient Out- comes on a KinAir Bed or EHOB Waffle Mattress. TriService Nursing Research Program (TSNRP), Bethesda, Maryland, USA. Collier, M.E., 1996. Pressure-reducing mattresses. Journal of Wound Care 5 (5), 207–211.
- 82. Conine, T.A., Daechsel, D., Lau, M.S., 1990. The role of alternating air and silicore overlays in preventing decubitus ulcers. International Journal of Rehabilitation Research 13 (1), 57–65. Conine, T.A., Daeschel, D., Hershler, C., 1993. Pressure sore prophylaxis in elderly patients using slab foam or customised contoured foam wheelchair cushions. Occupational Therapy Journal of Research 13 (2), 101–116. Conine, T.A., Hershler, C., Daechsel, D., Peel, C., Pearson, A., 1994. Pressure sore prophylaxis in elderly patients using polyurethane foam or Jay wheelchair cushions. International Journal of Rehabilitation Research 17 (2), 123–137. Cooper, P.J., Gray, D.G., Mollison, J., 1998. A randomised controlled trial of two pressure reducing surfaces. Journal of Wound Care 7 (8), 374–376. Daechsel, D., Conine, T.A., 1985. Special mattresses: effectiveness in preventing decubitus ulcers in chronic neurologic patients. Archives of Physical Medicine and Rehabilitation 66 (4), 246–248. Economides, N.G., Skoutakis, V.A., Carter, C.A., Smith, V.H., 1995. Evalua- tion of the effectiveness of two support surfaces following myocu-
- 83. taneous flap surgery. Advances in Wound Care 8 (1), 49–53. Essex, H.N., Clark, M., Sims, J., Warriner, A., Cullum, N., 2009. Health- related quality of life in hospital inpatients with pressure ulceration: assessment using generic health-related quality of life measures. Wound Repair and Regeneration 17 (6), 797–805. pean Pressure Ulcer Advisory Panel, National Pressure Ulcer Advi- sory Panel, 2009. Prevention and Treatment of Pressure Ulcers: hampered by small sample size and low quality. Future Euro E. McInnes et al. / International Journal of Nursing Studies 49 (2012) 345–359358 Quick Reference Guide. National Pressure Ulcer Advisory Panel, Washington, DC. Ewing, M., Garrow, C., Presley, T., Ashley, C., Kinsella, N., 1964. Further experiences in the use of sheep skins as an aid in nursing. The Australian Nurses’ Journal Sept 215–219. Exton-Smith, A.N., Overstall, P.W., Wedgewood, J., Wallace, G., 1982. Use of the ‘air wave system’ to prevent pressure sores in hospital. The Lancet 1 (8284), 1288–1290.
- 84. Feuchtinger, J., de Bie, R., Dassen, T., Halfens, R., 2006. A 4- cm thermo- active viscoelastic foam pad on the operating room table to prevent pressure ulcer during cardiac surgery. Journal of Clinical Nursing 15 (2), 162–167. Fox, C., 2002. Living with a pressure ulcer: a descriptive study of patients’ experiences. British Journal of Community Nursing 7 (10). Franks, P., Winterburg, J., Moffatt, C., 2002. Health-related quality of life and pressure ulceration assessment in patients treated in the com- munity. Wound Repair and Regeneration 10 (3), 133–140. Gallagher, S.M., 1997. Morbid obesity: a chronic disease with an impact on wound and related problems. Ostomy/Wound Management 43 (5) pp. 18–24, 26–17. Gebhardt, K.S., Bliss, M.R., Winwright, P.L., Thomas, J., 1996. Pressure relieving supports in an ICU. Journal of Wound Care 5 (3), 116–121. Gentilello, L., Thompson, D.A., Tonnesen, A.S., Hernandez, D., Kapadia, A.S., Allen, S.J., et al., 1988. Effect of a rotating bed on the incidence of pulmonary complications in critically ill patients. Critical Care Med-
- 85. icine 16 (8), 783–786. Geyer, M.J., Brienza, D.M., Karg, P., Trefler, E., Kelsey, S., 2001. A rando- mized control trial to evaluate pressure-reducing seat cushions for elderly wheelchair users. Advances in Skin and Wound Care 14 (3), 120–129. Gilcreast, D.M., Warren, J.B., Yoder, L.H., Clark, J.J., Wilson, J.A., Mays, M.Z., 2005. Research comparing three heel ulcer-prevention devices. Jour- nal of Wound Ostomy and Continence Nursing 32 (2), 112–120. Girouard, K., Harrison, M., VanDenKerkof, E., 2008. The symptom of pain with pressure ulcers: a review of the literature. Ostomy Wound Management 54 (5) pp. 30–40, 42. Goldstone, L., Norris, M., O’Reilly, M., White, J., 1982. A clinical trial of a bead bed system for the prevention of pressure sores in elderly orthopaedic patients. Journal of Advanced Nursing 7 (6), 545– 548. Gorecki, C., Brown, J., Nelson, E., Briggs, M., Schoonhoven, L., Dealey, C., 2009. European Quality of Life Pressure Ulcer Project group. Impact of pressure ulcers on quality of life in older patients: a systematic review. Journal of American Geriatric Society 57 (7), 1175– 1183. Graves, N., Birrell, F., Whitby, M., 2005a. Effect of pressure
- 86. ulcers on length of hospital stay. Infection Control Hospital Epidemiology 26 (3), 293–297. Graves, N., Birrell, F., Whitby, M., 2005b. Modelling the economic losses from pressure ulcers among hospitalized patients in Australia. Wound Repair and Regeneration 13 (5), 462–467. Gray, D.G., Campbell, M., 1994. A randomized clinical trial of two types of foam mattresses. Journal of Tissue Viability 4 (4), 128–132. Gray, D.G., Cooper, P.J., Campbell, M., 1998. A study of the performance of a pressure reducing foam mattress after three years of use. Journal of Tissue Viability 8 (3), 9–13. Gunningberg, L., Lindholm, C., Carlsson, M., Sjoden, P.O., 2000. Effect of visco-elastic foam mattresses on the development of pressure ulcers in patients with hip fractures. Journal of Wound Care 9 (10), 455–460. Hampton, S., 1997. Evaluation of the new Cairwave Therapy System in one hospital trust. British Journal of Nursing 6 (3), 167–170. Higgins, J.P.T., Altman, D.G., Sterne, J.A.C., 2011. Chapter 8: assessing risk of bias in included studies. In: Higgins, J.P.T., Green, S. (Eds.), Co- chrane Handbook for Systematic Reviews of Interventions
- 87. Version 5.1.0 [updated March 2011]. The Cochrane Collaboration. Available from <www.cochrane-handbook.org> Higgins, J.P.T., Thompson, S., Deeks, J., Altman, D.G., 2003. Measuring inconsistency in meta-analyses. BMJ 327 (7414), 557–560. Hofman, A., Geelkerken, R.H., Wille, J., Hamming, J.J., Hermans, J., Breslau, P.J., 1994. Pressure sores and pressure-decreasing mattresses: con- trolled clinical trial. Lancet 343 (8897), 568–571. Inman, K.J., Sibbald, W.J., Rutledge, F.S., Clark, B.J., 1993. Clinical utility and cost-effectiveness of an air suspension bed in the prevention of pressure ulcers. JAMA 269 (9), 1139–1143. Jolley, D.J., Wright, R., McGowan, S., Hickey, M.B., Campbell, D.A., Sinclair, R.D., et al., 2004. Preventing pressure ulcers with the Australian Medical Sheepskin: an open-label randomised controlled trial. Med- ical Journal of Australia 180 (7), 324–327. Junkin, J., Gray, M., 2009. Are pressure redistribution surfaces or heel protection devices effective for preventing heel pressure ulcers? Journal of Wound Ostomy Continence Nursing 36 (6), 602–608. Kemp, M.G., Kopanke, D., Tordecilla, L., Fogg, L., Shott, S., Matthiesen, V.,
- 88. et al., 1993. The role of support surfaces and patient attributes in preventing pressure ulcers in elderly patients. Research in Nursing and Health 16 (2), 89–96. Keogh, A., Dealey, C., 2001. Profiling beds versus standard hospital beds: effects on pressure ulcer incidence outcomes. Journal of Wound Care 10 (2), 15–19. Lahmann, N.A., Kottner, J., 2011. Relation between pressure, friction and pressure ulcer categories: a secondary data analysis of hospital patients using CHAID methods. International Journal of Nursing Studies, doi:10.1016/j.ijnurstu.2011.07.004. Langemo, D., Melland, H., Hanson, D., Olson, B., Hunter, S., 2000. The lived experience of having a pressure ulcer: a qualitative analysis. Advances in Skin and Wound Care 13, 225–235. Laurent, S., 1997. Effectiveness of pressure decreasing mattresses in cardiovascular surgery patients: a controlled clinical trial. In: 3rd European Conference for Nurse Managers, Brussels, Belgium, October, 1997. Lazzara, D.J., Buschmann, M.B.T., 1991. Prevention of pressure ulcers in elderly nursing home residents: are special support surfaces the answer? Decubitus 4 (4), 42–48. Lefebvre, C., Manheimer, E., Glanville, J., on behalf of the
- 89. Cochrane Information Retrieval Methods Group, 2009. Chapter 6: Searching for studies. In: Higgins, J.P.T., Green, S. (Eds.). Cochrane Handbook for Systematic Reviews of Interventions Version 5.0.2 [updated Septem- ber 2009]. The Cochrane Collaboration, 2009. Available from <www.cochrane-handbook.org>. Lim, R., Sirett, R., Conine, T.A., Daechsel, D., 1988. Clinical trial of foam cushions in the prevention of decubitis ulcers in elderly patients. Journal of Rehabilitation Research 25 (2), 19–26. McGowan, S., Montgomery, K., Jolley, D., Wright, R., 2000. The role of sheepskins in preventing pressure ulcers in elderly orthopaedic patients. Primary Intention 8 (4), 1–8. McInnes, E., Jammali-Blasi, A., Bell-Syer, S., Dumville, J., Cullum, N., 2011. Support surfaces for pressure ulcer prevention. Cochrane Database of Systematic Reviews Issue 4. Art. No.: CD001735. doi:10.1002/ 14651858.CD001735.pub4.f. Mistiaen, P., Francke, A., Achterberg, W., Ament, A., Halfens, R., Huizinga, J., 2009. Australian Medical Sheepskin is effective for the prevention of pressure ulcers. Tijdschrift voor Ouderengeneeskunde 5, 186–190. Mistiaen, P., Jolley, D., McGowen, S., Hickey, M.,
- 90. Spreeuwenberg, P., Francke, A., 2010. A multilevel analysis of three randomised con- trolled trials of Australian Medical Sheepskin in the prevention of sacral pressure ulcers. MJA 193 (11), 638–641. Moher, D.A., Tetzlaff, L., Altman, J., The PRISMA Group, 2009. Preferred Reporting Items for Systematic Reviews and Meta-Analyses: The PRISMA Statement. BMJ 339. National Institute for Clinical Excellence, 2003. Pressure Ulcer Prevention: Pressure Ulcer Risk Assessment and Prevention, including the Use of Pressure-Relieving Devices (Beds, Mattresses and Overlays) for the Prevention of Pressure Ulcers in Primary and Secondary Care. National Institute for Clinical Excellence, London. Nixon, J., Cranny, G., Iglesias, C., Nelson, E.A., Hawkins, K., Phillips, A., et al., 2006. Randomised, controlled trial of alternating pressure mattresses compared with alternating pressure overlays for the pre- vention of pressure ulcers: PRESSURE (pressure relieving support surfaces) trial. BMJ 332 (7555), 1413–1415. Nixon, J., McElvenny, D., Mason, S., Brown, J., Bond, S., 1998. A sequential randomised controlled trial comparing a dry visco-elastic polymer pad and standard operating table mattress in the prevention of
- 91. postoperative pressure sores. International Journal of Nursing Studies 35 (4), 193–203. Phillips, L., Buttery, J., 2009. Exploring pressure ulcer prevalence and preventative care. Nursing Times 105 (16), 34–36. Price, P., Bale, S., Newcombe, R., Harding, K., 1999. Challenging the pressure sore paradigm. Journal of Wound Care 8 (4), 187–190. Reddy, M., Gill, S., Rochon, P., 2006. Preventing pressure ulcers: a sys- tematic review. JAMA 296 (8), 974–984. Review Manager (RevMan) Version 5.0, 2008. The Nordic Cochrane Centre, The Cochrane Collaboration, Copenhagen. Rinda, L., Falce, R.L., 2002. Skin care in older people. Primary Health Care 12 (7), 51–57. Russell, J.A., Lichtenstein, S.L., 2000. Randomised controlled trial to determine the safety and efficacy of a multi-cell pulsating dynamic mattress system in the prevention of pressure ulcers in patients undergoing cardiovascular surgery. Ostomy/Wound Management 46 (2) pp. 54–45 46–51. Russell, L., Reynolds, T.M., Carr, J., Evans, A., Holmes, M., 2000. Rando- mised controlled trial of two pressure-relieving systems. Journal
- 92. of Wound Care 9 (2), 52–55. http://www.cochrane-handbook.org/ http://dx.doi.org/10.1016/j.ijnurstu.2011.07.004 http://www.cochrane-handbook.org/ Russ San Sant Schu Schu Scot Side Spoe Stap Sum E. McInnes et al. / International Journal of Nursing Studies 49 (2012) 345–359 359 ell, L.J., Reynolds, T.M., Park, C., Rithalia, S., Gonsalkorale, M., Birch, J., et al., 2003. Randomised clinical trial comparing CONFOR-Med and standard hospital mattresses: results of the prevention of pressure
- 93. ulcers study (PPUS-1). Advances in Skin and Wound Care 16 (6), 317–327. ada, H., Sugama, J., Matsui, Y., Konya, C., Kitagawa, A., Okuwa, M., et al., 2003. Randomised controlled trial to evaluate a new double-layer air-cell overlay for elderly patients requiring head elevation. Journal of Tissue Viability 3, 112–114 (13 (3),116, 118 passim). y, J.E., Butler, M.K., Whyman, J.D., 1994. A Comparison Study of 6 Types of Hospital Mattress to Determine Which Most Effectively Reduces the Incidence of Pressure Sores in Elderly Patients with Hip Fractures in a District General Hospital. . ltz, A., Bien, M., Dumond, K., Brown, K., Myers, A., 1999. Etiology and incidence of pressure ulcers in surgical patients. AORN Journal 70 (3) pp. 443–439 434, 437–440. ltz, A.A., 1998. Study results: prediction and prevention of pressure ulcers in surgical patients. Advances in Wound Care 11 (3 Suppl) 11–11. tish Intercollegiate Guidelines Network, 2009. Search filters. http:// www.sign.ac.uk/methodology/filters.html#random. ranko, S., Quinn, A., Burns, K., Froman, R.D., 1992. Effects of position and mattress overlay on sacral and heel pressures in a clinical population. Research in Nursing and Health 15 (4), 245–251.
- 94. lhof, G.D., 2000. Management of pressure ulcers in the nursing home. Annals of Long Term Care 8 (8), 69–77. leton, M., 1986. Preventing pressure sores—an evaluation of three products. . . foam, ripple pads, and Spenco pads. Geriatric Nursing (London, England) 6 (2), 23–25. mer, W.R., Curry, P., Haponikm, E.F., Nelson, S., Elston, R., 1989. Continuous mechanical turning of intensive care unit patients short- ens length of stay in some diagnostic-related groups. Journal of Critical Care 4, 45–53. Takala, J., Varmavuo, S., Soppi, E., 1996. Prevention of pressure sores in acute respiratory failure: a randomised controlled trial. Clinical Inten- sive Care 7 (5), 228–235. Taylor, L., 1999. Evaluating the Pegasus Trinova: a data hierarchy approach. British Journal of Nursing 8 (12), 771–778. Theaker, C., Kuper, M., Soni, N., 2005. Pressure ulcer prevention in intensive care—a randomised control trial of two pressure- relieving devices. Anaesthesia 60 (4), 395–399. Thomas, D.R., 2001. Improving outcomes of pressure ulcers with nutri- tional interventions: a review of the evidence. Nutrition 17, 121–125.
- 95. Tymec, A.C., Pieper, B., Vollman, K., 1997. A comparison of two pressure relieving devices on the prevention of heel pressure ulcers. Advances in Wound Care 10 (1), 39–44. Vanderwee, K., Clark, M., Dealey, C., Gunningberg, L., Defloor, T., 2007a. Pressure ulcer prevalence in Europe: a pilot study. Journal of Evalua- tion in Clinical Practice 13 (2), 227–235. Vanderwee, K., Grypdonck, M.H., De Bacquer, D., Defloor, T., 2007b. Effectiveness of turning with unequal time intervals on the incidence of pressure ulcer lesions. Journal of Advanced Nursing 57 (1), 59–68. Vanderwee, K., Grypdonck, M.H., Defloor, T., 2005. Effectiveness of an alternating pressure air mattress for the prevention of pressure ulcers. Age and Ageing 34 (3), 261–267. Van Gilder, C., Amlung, S., Harrison, P., Meyer, S., 2009. Results of the 2008–2009 International Pressure Ulcer Prevalence Survey and a 3- year, acute care, unit-specific analysis. Ostomy/Wound Management 55 (11), 39–45. Vyhlidal, S.K., Moxness, D., Bosak, K.S., Van Meter, F.G., Bergstrom, N., 1997. Mattress replacement or foam overlay? A prospective study on
- 96. the incidence of pressure ulcers. Applied Nursing Research 10 (3), 111–120. Whitney, J.D., Fellows, B.J., Larson, E., 1984. Do mattresses make a difference? Journal of Gerontological Nursing 10 (9), 20–25. Woodbury, M., Houghton, P., 2004. Prevalence of pressure ulcers in Canadian healthcare settings. Ostomy/Wound Management 50 (10) pp. 22–24, 26, 28, 30, 32, 34, 36–28. http://www.sign.ac.uk/methodology/filters.html http://www.sign.ac.uk/methodology/filters.htmlPreventing pressure ulcers-Are pressure-redistributing support surfaces effective? A Cochrane systematic review and meta- analysisIntroductionMethodsResultsComparisons: ‘low-tech’ constant low pressure support surfacesComparisons between ‘low-tech’ constant low pressure support surfaces and standard foam surfacesComparisons between alternative foam support surfacesOther ‘low-tech’ support surfaces with various comparisonsComparisons: ‘high-tech’ pressure support surfacesComparisons between alternating pressure supports and standard hospital mattressComparisons between alternating pressure supports and constant low pressure supportsComparisons between different alternating pressure devicesLow-air-loss and air-fluidised bedsComparisons between other pressure supportsOperating table overlaysKinetic turning tables and profiling bedsSeat cushionsDiscussionStrengths and limitationsConclusionReferences