Research Critique Guidelines – Part IUse this docume.docx
1. Research Critique Guidelines – Part I
Use this document to organize your essay. Successful
completion of this assignment requires that you provide a
rationale, include examples, and reference content from the
studies in your responses.
Qualitative Studies
Background of Study
1. Summary of studies. Include problem, significance to
nursing, purpose, objective, and research question.
How do these two articles support the nurse practice issue you
chose?
1. Discuss how these two articles will be used to answer your
PICOT question.
2. Describe how the interventions and comparison groups in the
articles compare to those identified in your PICOT question.
Method of Study:
1. State the methods of the two articles you are comparing and
describe how they are different.
2. Consider the methods you identified in your chosen articles
and state one benefit and one limitation of each method.
Results of Study
1. Summarize the key findings of each study in one or two
comprehensive paragraphs.
2. What are the implications of the two studies in nursing
practice?
Ethical Considerations
1. Discuss two ethical consideration in conducting research.
2. Describe how the researchers in the two articles you choose
3. care of prevention. However, there were limitations to some
studies and further research is needed to confirm the role of
silicone foam dressings.
Keywords: pressure ulcers, silicone dressings, preventive
medicine, hospital acquired infection, pressure sores, decubitus
ulcer
Go to:
Introduction and background
Pressure ulcers, also called pressure sores or bedsores, are a
burden to healthcare and have a significant cost of morbidity. In
2013, a United States Medicare study reported the incidence of
hospital-acquired pressure ulcers to be 4.5% in hospitalized
patients, with an estimated 11 billion dollars for the cost of
pressure ulcer care [1-2].
Pressure ulcers are due to a multitude of factors that contribute
to tissue vulnerability and breakdown. In 2007, the National
Pressure Ulcer Advisory Panel (NPUAP) established a staging
system for categorizing pressure ulcer injuries. Pressure ulcers
are often formed where skin covers bony areas and common
sites are the back of the head and ears, the shoulders, the
elbows, the lower back and buttocks, the hips, the inner knees,
and the heels. Although pressure ulcers can develop over the
course of 24 hours, they may not present until a week later.
Stage I pressure ulcers present with intact, erythematous skin
that does not blanch. Stage II pressure ulcers can appear as a
fluid-filled blister, which represents breakage of the epidermis
and may involve the underlying dermis. Stage III pressure
ulcers present with necrotic tissue and extend into the
subcutaneous tissue. Finally, Stage IV pressure ulcers extend
deep into the bone or muscle with full thickness tissue loss [3].
The incidence and prevalence of pressure ulcers vary greatly,
depending on the setting. Patients hospitalized in the intensive
care unit (ICU) or immobilized after major surgery are at higher
risk [4]. Vigilant patient care teams educated in pressure ulcer
care can identify the signs of tissue breakdown and are aware of
4. the numerous factors that place patients at risk of pressure ulcer
formation, including reduced mobility, nutritional status, urine
or fecal incontinence, medications that cause reduced sensation
and immobility, instruments and tools that create mechanical
pressure against the body, and conditions that decrease tissue
oxygenation [3].
Barrier creams used in the prevention of pressure ulcers form a
protective layer that keeps away excessive moisture due to
incontinence, perspiration, or wound drainage and aid in
maintaining the integrity of the skin [5]. These creams include
Calmoseptine® (Calmoseptine, Inc., Huntington Beach, CA),
Lantiseptic® (Santus, Duluth, GA), Silvadene® (Pfizer, Inc.,
New York, NY), and others that use silver sulfadiazine, zinc
oxide, or lanolin as active ingredients to prevent infection. A
hydrocolloid dressing normally used in wound care, such as
Tegaderm® (3M Center, St. Paul, MN), is also frequently used
in combination with barrier creams and contains an adhesive
compound in combination with a water-resistant outer layer to
prevent additional moisture exposure [6]. Silicone foam
dressings, such as Mepilex® (Mölnlycke Health Care,
Gothenburg, Sweden), are soft silicone multi-layered foam
dressings that contain silver, which acts as an antibiotic agent,
and an adhesive material different from the regularly used
hydrocolloids that result in less skin abrasion when it is time to
remove and replace the dressing [7].
Currently, standard protocols for care in pressure ulcer
prevention vary between hospital systems with different
algorithms for inpatient and outpatient situations but include the
use of low-pressure beds, positioning and turning, and barrier
cream with a hydrocolloid layering placed over the area of
application in areas at risk of pressure formation, such as the
sacrum, heels, and buttocks [3]. Although the standard care has
been effective, a newer material, silicone foam dressing, has
been introduced as an alternative for pressure ulcer prevention
with potentially greater cost and health benefits for hospitals
and patients, respectively [8]. If the silicone foam dressings are,
5. indeed, better at treating and preventing sore formation in
immobilized patients, then nurses should also benefit in their
role as patient caregivers by being able to provide greater and
more efficient care to their patients.
This literature review will examine whether immobilized
patients in the hospital setting who are given silicone foam
dressings compared to the standard protocol, which utilizes
barrier creams under a hydrocolloid layering for the prevention
of pressure ulcer, have an effect on the incidence of Stage I
pressure ulcer formation.
Go to:
Review
A literature review was conducted to determine the
effectiveness of standard protocols for pressure ulcer care
versus a newer silicone foam dressing. PubMed searches were
performed using the phrases “silicone foam dressing” and
“barrier creams” in the English language with the modifier of
articles published in the last seven years. Articles were then
screened for relevance and excluded if the studies were not
primarily focused on pressure ulcer prevention. This search
process yielded five quantitative research articles focusing on
the usage and effectiveness of silicone foam dressings.
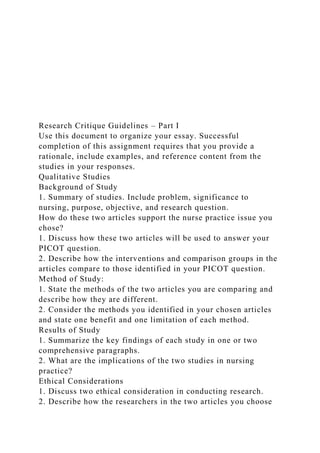
This review covers the five separate studies at various
institutions detailing the utility and benefits of using silicone
foam dressing as an alternative to the standard care of pressure
ulcer prevention (Table (Table1).1). Huang, et al. sought to
determine if there was any way to reduce the incidence of nasal
pressure ulcers that arise as a complication of nasotracheal
intubation during oral and maxillofacial surgery [6]. By using
an initial animal model to test the clinical application of
silicone foam material as a means of reducing pressure on the
nasal area, Huang, et al. believed that the use of the cushioning
material would aid in protection during intubation as opposed to
intubation without additional cushion protection. Eighteen
patients were studied. The results showed a decrease in the size
6. of nasal pressure sores between the control and comparison
groups to which Huang, et al. attributed to the protective
efficacy of the silicone foam dressing used as lining during
nasal intubation. It should be noted, however, that only a small
sample size of 18 participants was included in this study.Table
1
Study Characterisitics
n = number
Publication Date, Authors
Location, Setting, n
Body Site Reported/Stage of Ulcer
Study Design
Pressure Ulcer Prophylactic
Findings
(2009) Huang, et al. [6]
Dalin, Taiwan, Republic of China, Buddhist Dalin Tzu Chi
General Hospital operating room, n = 18
Nose/ Stage I
Quantitative prospective cohort study. Patients in the study
group had foam surrounding their intubation tubes compared to
the control group who did not.
Silicone foam dressing vs standard hospital treatment protocol
from Tzu Chi General Hospital.
Silicone foam dressings were found to reduce the incidence of
pressure ulcer formation due to nasotracheal tube intubation.
8/8 (100%) formed pressure ulcers in the control group while
6/10 (60%) in the intervention group formed pressure ulcers.
(2011) Forni, et al. [9]
Italy, Rizzoli Orthopedic Institute, n = 105
Heel/ Stage I
Quantitative prospective cohort study. Patients in the
intervention group were compared to control group data
collected in the previous year.
Silicone foam dressing vs standard hospital treatment protocol
from Rizzoli Orthopedic Institute.
Pressure ulcer reduction in patients wearing casts was possible
7. using silicone foam dressings placed within the cast with 2/56
(3.6%) forming pressure ulcers compared to the control group
incidence rate of 21/49 (42.9%).
(2012) Brindle and Wegelin [4]
Virginia, Virginia Commonwealth University Medical Center
ICU, n = 85
Sacrum/Stage I
Quantitative prospective cohort study. Intervention group was
given Mepilex® Border Sacrum dressings with standard care
protocol compared to control group, which only received
standard care protocol
Silicone foam dressing vs standard hospital treatment protocol
from Virginia Commonwealth University Medical Center
Patients undergoing cardiac surgery who were given silicone
foam dressings after surgery had pressure ulcer formation
incidence of 1/50 (2%) compared to the control group who did
not receive the silicone foam dressing 4/35 (11.4%). The
findings were not statistically significant, however, due to
sample size.
(2012) Chaiken [11]
Illinois, Swedish Covenant Hospital ICU, n = 563
Sacrum/Stage I
Quantitative prospective cohort study. Patients in the study
group were compared to those in the control group data
collected the previous year.
Silicone foam dressing vs standard hospital treatment protocol
from Swedish Covenant Hospital.
Reduction of sacral pressure ulcers was found in the
intervention group with 5/273 (1.8%) incidence of pressure
ulcer formation compared to 36/291 (12.3%) in the control
group.
(2015) Santamaria, et al. [12]
Australia, Royal Melbourne Hospital ICU n = 313
Sacrum/ heel/Stage I
Randomized controlled trial with the intervention group
receiving Mepilex® Border Sacrum and Mepilex® Heel
8. dressings. Both groups received standard prevention strategies.
Silicone foam dressing vs standard hospital treatment protocol
from Royal Melbourne Hospital.
There was a significantly decreased formation of pressure ulcers
in the intervention group in comparison to the control group
who received traditional wound dressing. 5/161 (3.1%)
developed pressure ulcers in the intervention group vs 20/152
(13.1%) in the control group.
Open in a separate window
Forni, et al. investigated pressure ulcer prevention by using
foam dressings in patients with cast immobilization [9]. One
hundred and fifty-six patients were included in this study, 85 in
the control group and 71 in the experimental group. Inclusion
criteria included any patient admitted to an Italian orthopedic
research hospital for an orthopedic associated disease requiring
a plaster cast of their foot. The results provided substantial
evidence of pressure ulcer prevention by applying foam within
the plaster cast of patients with data that was statistically
significant for differences among the control and experimental
groups. Forni, et al. discussed the positive impact that foams
can have as a deterrent against pressure ulcers in patients
requiring casts as well as its potential use in diabetics who are
more prone to developing pressure ulcers [9].
Cardiac surgery patients are one of the most at-risk patient
populations in the incidence of hospital-acquired pressure ulcers
[10]. In 2012, Brindle and Wegelin hypothesized that using
Mepilex®, a silicone foam dressing, around the area of the
sacrum in these patients would decrease incidence rates of
pressure ulcer formation in comparison to the hospital’s current
standard care, which consisted of the use of a skin protectant,
Calmoseptine®, on high risk areas [4]. Silicone foam dressing
impregnated with silver as an antibiotic was the independent
variable in the study, while the dependent variable was the
formation of pressure ulcers in the area of the sacrum. A total of
85 patients were enrolled in this study who had met the criterion
for inclusion and exclusion. Eligibility for the study included
9. patients who had undergone a surgical procedure within a
certain period of time, cardiac arrest on admission, in shock, or
had some sort of condition that required chronic bed rest.
Statistical analyses for the variables collected showed no
significant differences when compared between the
experimental versus the control groups. Results showed that the
incidence rate of pressure ulcer formation in patients who were
given Mepilex® silicone foam dressing was not considerably
less than in patients who were given the barrier cream. Brindle
and Wegelin concluded in their paper that, while using silicone
foam dressings did produce a decreased incidence rate in
pressure ulcers in the intervention group, it was not by much in
comparison to the control group. They reasoned that the smaller
sample size than what was originally planned, in addition to the
standard care procedures and attentive efforts of the ICU nurses
in patient treatment, may have played a part in the findings of
the study.
In 2012, Chaiken, in a similar study, sought to determine
whether the incidence of pressure ulcer formation would
decrease in the ICU through the use of silicone foam dressing
placed at the area of the sacrum [11]. During the prospective
experiment, Mepilex® Border Sacrum, a type of silicone foam,
was given to a group of 273 newly admitted patients in the ICU
with nurses instructed in changing the dressing twice a week
while following the hospital's standard protocol for pressure
ulcer prevention. The study took place over a six-month period
and the results showed a decrease in the incidence rates of
pressure ulcers from 12.3% during the 35-month observation
period in the comparison group to 1.8% in the experiment
group. In addition to the lower incidence rate of pressure ulcers,
Chaiken further reported an average expenditure of $6,653.00
for the six-month experiment period, which, in turn, saved the
hospital money by avoiding the higher cost of treatment
associated with treating pressure ulcers.
In 2013, Santamaria, et al. examined the effectiveness of soft
silicone dressings of the sacrum and the heel of the body in the
10. ICU setting in preventing pressure ulcers [12]. This randomized
control study included 440 patients who were newly admitted to
the emergency department and were subsequently transferred to
the ICU. Findings were significant for decreased formation of
pressure ulcers in the intervention group, as measured by the
Australian Wound Management Association (AWMA) four-
point grading system, in comparison to the control group who
received a standard barrier cream with a hydrocolloid layering.
Santamaria, et al. concluded that use of silicone foam dressings
in combination with thorough risk assessment and evidence-
based pressure ulcer prevention strategies had a substantial
impact on the reduction of pressure ulcer incidence.
Upon review of the articles, there is efficacy and utility of
silicone foam dressings among other forms of barriers in the
prevention of pressure ulcers. This literature review shows that
standard traditional methods were helpful in preventing pressure
ulcers, but silicone foam dressings were even more effective in
reducing the incidence of pressure ulcer formation (3.6% versus
42.9% in the study conducted by Forni, et al.) [9]. Not only
should silicone foam dressings be considered due to their
effectiveness, Santamaria, et al. concluded in their study that
they should be considered due to their economic savings to
health care institutions (average net cost of intervention
compared to control, $52.87 versus $107.91) [12]. There were
still limitations, which were evident when reviewing the
literature, even though each article provided evidence regarding
the effectiveness of silicone foam dressings. Research
conducted by Huang, et al. provided information regarding
protection of pressure ulcer formation, but the paper did not
include the methods of data collection or methods of analyses
[6]. The research by Forni, et al. and Chaiken was limited by a
lack of a parallel control within these respective studies and
used past patient data as a control instead [9, 11]. Brindle and
Wegelin mentioned that a major limitation of their study was
indeed the duration of the experiment and sample size [4].
Go to:
11. Conclusions
We would like to recommend that future research would not
only benefit from increasing the sample size and diversifying
the population but should strive to conduct trials over longer
periods of time in order to obtain adequate data and use the
maximal amount of data it can for analysis. Additionally, the
research may be expanded to other clinical areas where the
incidence of pressure ulcer formation is high, such as patients
with incontinence, recurrent pressure ulcers, and the elderly
hospitalized with altered mental status.
Proper skin care is very important in the prevention of these
ulcers. Even though guidelines are in place for the prevention of
pressure ulcers, the incidence is still very high in patients who
are in the ICU or who have had major surgeries. Prevention is
extremely important because not only does the patient suffer
from the pressure ulcer, but there is an economic impact related
to them as the hospital may incur additional costs related to
pressure ulcer management. In addition to standard protocols,
the use of silicone foam dressings as a barrier against irritation
and constant pressure to the skin should be effectively utilized
in pressure ulcer prevention.
Go to:
Notes
The content published in Cureus is the result of clinical
experience and/or research by independent individuals or
organizations. Cureus is not responsible for the scientific
accuracy or reliability of data or conclusions published herein.
All content published within Cureus is intended only for
educational, research and reference purposes. Additionally,
articles published within Cureus should not be deemed a
suitable substitute for the advice of a qualified health care
professional. Do not disregard or avoid professional medical
advice due to content published within Cureus.
Go to:
12. Footnotes
A research grant and supply of dressings was provided by a
Mepilex® supplier in one of the studies cited within this article.
Go to:
References
1. US Medicare data show incidence of hospital-acquired
pressure ulcers is 4.5%, and they are associated with longer
hospital stay and higher risk of death. Moore Z. Evid Based
Nurs. 2013;16:118–119. [PubMed] [Google Scholar]
2. An economic analysis of repositioning for the prevention of
pressure ulcers. Moore Z, Cowman S, Posnett J. J Clin
Nurs. 2013;22:2354–2360. [PubMed] [Google Scholar]
3. Pressure ulcers: what clinicians need to know. Wake
WT. http://www.ncbi.nlm.nih.gov/pmc/articles/PMC2912087/ P
erm J. 2010;14:56–60. [PMC free article][PubMed] [Google
Scholar]
4. Prophylactic dressing application to reduce pressure ulcer
formation in cardiac surgery patients. Brindle CT, Wegelin
JA. J Wound Ostomy Continence Nurs. 2012;39:133–
142. [PubMed] [Google Scholar]
5. An economic evaluation of four skin damage prevention
regimens in nursing home residents with incontinence:
economics of skin damage prevention. Bliss DZ, Zehrer C,
Savik K, Smith G, Hedblom E. J Wound Ostomy Continence
Nurs. 2007;34:143–152. [PubMed] [Google Scholar]
6. Preventing pressure sores of the nasal ala after nasotracheal
tube intubation: from animal model to clinical application.
Huang TT, Tseng CE, Lee TM, Yeh JY, Lai YY. J Oral
Maxillofac Surg. 2009;67:543–551. [PubMed] [Google Scholar]
7. Mepilex® Ag: an antimicrobial, absorbent foam dressing with
Safetac® technology. Barrett S. http://less-
pain.com/documents/evidence/BarretS_BritishJournalofNursing
2009.pdf Br J Nurs. 2009;18:S28, S30-6. [PubMed] [Google
Scholar]
13. 8. Cost-effectiveness analysis in comparing alginate silver
dressing with silver zinc sulfadiazine cream in the treatment of
pressure ulcers. Chuangsuwanich A, Chortrakarnkij P,
Kangwanpoom J. Arch Plast Surg. 2013;40:589–596. [PMC free
article] [PubMed] [Google Scholar]
9. Use of polyurethane foam inside plaster casts to prevent the
onset of heel sores in the population at risk. A controlled
clinical study. Forni C, Loro L, Tremosini M, Mini S, Pignotti
E, Bigoni O, Guzzo G, Bellini L, Trofa C, Di Cataldo AM,
Guzzi M. J Clin Nurs. 2011;20:675–680. [PubMed] [Google
Scholar]
10. The incidence of pressure ulcers in surgical patients of the
last 5 years: a systematic review. Chen HL, Chen XY, Wu
J. http://www.woundsresearch.com/article/incidence-pressure-
ulcers-surgical-patients-last-5-years-systematic-
review. Wounds. 2012;24:234–241. [PubMed] [Google Scholar]
11. Reduction of sacral pressure ulcers in the intensive care unit
using a silicone border foam dressing. Chaiken
N. http://journals.lww.com/jwocnonline/Abstract/2012/03000/R
eduction_of_Sacral_Pressure_Ulcers_in_the.4.aspx. J Wound
Ostomy Continence Nurs. 2012;39:143–145. [PubMed] [Google
Scholar]
12. A randomised controlled trial of the effectiveness of soft
silicone multi-layered foam dressings in the prevention of sacral
and heel pressure ulcers in trauma and critically ill patients: the
border trial. Santamaria N, Gerdtz M, Sage S, McCann J,
Freeman A, Vassiliou T, De Vincentis S, Ng AW, Manias E, Liu
W, Knott J. Int Wound J. 2015;12:302–308. [PubMed] [Google
Scholar]
Articles from Cureus are provided here courtesy of Cureus Inc.
Formats:
· Article
|
· PubReader
14. |
· ePub (beta)
|
· PDF (115K)
|
· Citation
Share
· Facebook
· Twitter
· Google+Save items
Add to FavoritesView more optionsSimilar articles in PubMed
· Role of multi-layer foam dressings with Safetac in the
prevention of pressure ulcers: a review of the clinical and
scientific data.[J Wound Care. 2016]
· A randomised controlled trial of the effectiveness of soft
silicone multi-layered foam dressings in the prevention of sacral
and heel pressure ulcers in trauma and critically ill patients: the
border trial.[Int Wound J. 2015]
· The cost-benefit of using soft silicone multilayered foam
dressings to prevent sacral and heel pressure ulcers in trauma
and critically ill patients: a within-trial analysis of the Border
Trial.[Int Wound J. 2015]
· Clinical effectiveness of a silicone foam dressing for the
prevention of heel pressure ulcers in critically ill patients:
Border II Trial.[J Wound Care. 2015]
· The use of prophylactic dressings in the prevention of pressure
ulcers: a literature review.[Br J Community Nurs. 2017]
See reviews...See all...Links
· Cited in Books
· MedGen
· PubMed
· TaxonomyRecent Activity
ClearTurn Off
· Pressure Ulcer Prevention in the Hospital Setting Using
Silicone Foam Dressings
15. Pressure Ulcer Prevention in the Hospital Setting Using
Silicone Foam Dressings
Cureus. 2016 Aug; 8(8)
· The Levels of Evidence and their role in Evidence-Based
Medicine
The Levels of Evidence and their role in Evidence-Based
Medicine
NIHPA Author Manuscripts. 2011 Jul; 128(1)305
· Generalizability
Generalizability
Neurology. 2012 Jun 5; 78(23)1886
· Pressure Ulcers: A Patient Safety Issue - Patient Safety and
Quality
Pressure Ulcers: A Patient Safety Issue - Patient Safety and
Quality
· Staffing and Quality of Care in Hospitals - Nursing Staff in
Hospitals and Nursi...
Staffing and Quality of Care in Hospitals - Nursing Staff in
Hospitals and Nursing Homes
See more...
· Prophylactic dressing application to reduce pressure ulcer
formation in cardiac surgery patients.[J Wound Ostomy
Continence Nurs. 2012]
· Pressure ulcers: what clinicians need to know.[Perm J. 2010]
· An economic evaluation of four skin damage prevention
regimens in nursing home residents with incontinence:
economics of skin damage prevention.[J Wound Ostomy
Continence Nurs. 2007]
· Preventing pressure sores of the nasal ala after nasotracheal
tube intubation: from animal model to clinical application.[J
Oral Maxillofac Surg. 2009]
· Review Mepilex Ag: an antimicrobial, absorbent foam
dressing with Safetac technology.[Br J Nurs. 2009]
· Pressure ulcers: what clinicians need to know.[Perm J. 2010]
· Cost-effectiveness analysis in comparing alginate silver
dressing with silver zinc sulfadiazine cream in the treatment of
16. pressure ulcers.[Arch Plast Surg. 2013]
· Preventing pressure sores of the nasal ala after nasotracheal
tube intubation: from animal model to clinical application.[J
Oral Maxillofac Surg. 2009]
See links ...
· Use of polyurethane foam inside plaster casts to prevent the
onset of heel sores in the population at risk. A controlled
clinical study.[J Clin Nurs. 2011]
· The incidence of pressure ulcers in surgical patients of the last
5 years: a systematic review.[Wounds. 2012]
· Prophylactic dressing application to reduce pressure ulcer
formation in cardiac surgery patients.[J Wound Ostomy
Continence Nurs. 2012]
· Reduction of sacral pressure ulcers in the intensive care unit
using a silicone border foam dressing.[J Wound Ostomy
Continence Nurs. 2012]
· A randomised controlled trial of the effectiveness of soft
silicone multi-layered foam dressings in the prevention of sacral
and heel pressure ulcers in trauma and critically ill patients: the
border trial.[Int Wound J. 2015]
· Use of polyurethane foam inside plaster casts to prevent the
onset of heel sores in the population at risk. A controlled
clinical study.[J Clin Nurs. 2011]
· A randomised controlled trial of the effectiveness of soft
silicone multi-layered foam dressings in the prevention of sacral
and heel pressure ulcers in trauma and critically ill patients: the
border trial.[Int Wound J. 2015]
· Preventing pressure sores of the nasal ala after nasotracheal
tube intubation: from animal model to clinical application.[J
Oral Maxillofac Surg. 2009]
· Reduction of sacral pressure ulcers in the intensive care unit
using a silicone border foam dressing.[J Wound Ostomy
Continence Nurs. 2012]
· Prophylactic dressing application to reduce pressure ulcer
formation in cardiac surgery patients.[J Wound Ostomy
Continence Nurs. 2012]
17. Support CenterSupport Center
RUNNING HEAD: THE PREVALENCE OF PRESSURE
ULCER AND PRESSURE INJURY
7
The Prevalence of Pressure Ulcer and Pressure Injury in the
Hospital & Skilled Nursing Facility
The Prevalence of Pressure Ulcer and Pressure Injury in the
Hospital & Skilled Nursing Facility
NAME
Grand Canyon University
June 1, 2019
Background of Study
The research indicates that hospital-acquired pressure injury(
HAPI) has been on the decline in America between 2010 and
18. 2014 as a result of efforts by Medicaid and Medicare services
as well as the Agency for Healthcare Research and Quality. In
the study by (Rondinelli, Zuniga, Kipnis, Kawar, llu, & Escobar
2018) the background information shows that the study
establishes that despite health care institutions having reduced
rates of hospital-acquired pressure injuries, the situation is not
eliminated. Resultantly, there is need for assessment in both
health service and nursing research. The objective of the study
is to offer a description of HAPI incidence, risk-adjusted
hospital variation, and risk factors within the contemporary
integrated healthcare system of California among 35- hospital
inpatient cohort. The focus was given to Kaiser Permanente
with conceptual consideration of immobility, tissue tolerance,
decreased activity, change in sensation, and immobility. Other
aspects like acute illness and chronic conditions. The study
offers the following significance to the study to enhance
understanding of HAPI, what causes it, and the prevalence
cases.
Pressure ulcer (PU) is caused by multiple factors and its
pathogenesis shows a multifactorial process that involved
hormonal changes, inflammatory aspects, impaired blood
perfusion, degenerative changes, and reduced immune
protection. A disturbingly rising situation in PU cases among
the old especially those who suffer from frailty and chronic
illnesses calls for higher awareness of therapeutic and
preventive measures like protecting the bony areas with pads
and repositioning every 2 hours to combat this. In the second
study conducted by Jaul, Barron, Rosenzwig, Menczel (2018)
reports that among the elderly, pressure ulcers are prevalent,
and they continue to rise as well as increase costs especially on
the older adults who ail from chronic diseases. The study
observes that currently there is a high level of awareness to
extensive, preventive, and therapeutic processes for treating
pressure ulcers with internal risk factors being comorbidities
that agreeably increase pressure ulcers. The study pays
19. attention to common chronic illnesses such as diabetes,
cardiovascular complications, renal diseases, chronic pulmonary
complications, and neurodegenerative disorders. Besides,
conditions such as anemia, malnutrition, incontinence,
disability, frailty, and hospitalization are essential in the multi-
disciplinary study of PU in old patients. The objective of the
research is to offer a description of acute and chronic conditions
that are risk aspects in elder patients for developing PU.
How do these two articles support the nurse practice issue I
chose?
The first article by Rondinelli et al. (2018) assists the study by
answering the PICOT because it shows the prevalence of HAPI
in healthcare as related causes. On the other hand, the second
study inquiries into the prevalence of PU among elder patients
are how risk factors increase such cases. Both studies have a
relevant objective that answers the PICOT question of the
study.
Method of Study:
In the first article, the method the study used was a
longitudinal analysis of retrospective inpatient episodes for
patients who were hospitalized between January 1st, 2013 and
June 30th, 2015 (Rondinelli et al., 2018). The key outcome was
the emergence of a HAPI over time. Among the predictors in the
case included HAPI risk factors using the Comorbidity Point
Score, the severity of illness through the Laboratory-Based
Acute Physiology Score, and the Braden Scale for predicting
Ulcer risk. There was the observation of the patients and
documentation of information on HAPI across the 35 hospitals.
On the contrary, in the second study by Jaul, Barron,
Rosenzwig, Menczel (2018), there is an overview of
comorbidities with PU in three diverse patient settings which
are the acute hospital, community, and long-term health care
with patients who have chronic diseases, old, and with pressure
ulcer grade 2 and over. The study too relied on the European
and National Pressure Ulcer Advisory Panels’ conceptual
framework, which covers indirect, potential, and direct causal
20. risk factors, it becomes possible to assess chronic illnesses to
determine the risk factors of chronic conditions and
complicating situation that possibly have an impact to the risk
for the development of PU.
Results of Study
From the first article by Rondinelli et al. (2018), it is indicated
that out of an analysis that involved 1661 HAPI inpatients and
726,605 non-HAPI episodes, the HAPI prevalence was 0.57
among 1,000 patient days which is 0.2 percent of episodes.
There were a significant protective HRs among female patients
who were in the emergency room for a medical cause. It means
an age, the severity of illness, comorbidity indexes, and the
Braden score as essential predictors of the HAPI prevalence.
The study indicates that HAPIs is fertile ground for research
and quality improvements plans. Furthermore, the use of
patients within the same context offered low baseline HAPI
incidence, meaning in future studies there should be a
recalibration of the model. The inclusion of diabetes led to a
nonsignificant HR for a predictor that has a strong association
with HAPI. Therefore, future studies require to analyze the
administrative, hospital, and staffing aspects that can quantify
the incidence-based interventions and how they impact on HAPI
incidences. An exploration of large data sets, the potential of
EMR-generated composing scores, and predictive analytics are
necessary. Besides, comorbidity burden score, Braden Scales
scores, and severity-of-illness scores are important here. There
is substantial inter-hospital variation in HAPI incidence a
situation remarkable where variables are included.
The results in the second study by Jaul, Barron, Rosenzwig,
Menczel (2018) it is shown that advanced heart disease where
there is low cardiac output and/or decreased oxygenation,
impact in situations of blood perfusion and peripheral ischemia
that contribute to the emergence of PU. When a patient has
cerebrovascular accidents or dehydration or edema, then there
are higher chances of having PU. With diabetes, a patient lacks
sensory perception from diabetic neuropathy, hence non-healing
21. wounds occur especially on the foot. Other vascular
complications and pressure When people age, pulmonary
functions go down, there is a decline in vital capacity, increase
in airway dead space and a decline in hypoxia, ventilatory
response which reduce lung functioning. Moreover, the issues of
inflammation, advanced pulmonary disease cause PU. The
prevention of PU among adults with severe pulmonary illnesses,
calls for management of edema, minimization of bedrest while
ill, optimization of nutrition, and optimization of endurance and
activity.
For patients with a decline in the functioning of the kidney in
aged individuals after the glomerular filtration rate and renal
blood flow declines. More illnesses like hypertension and
diabetes increase impaired kidney functioning cause issues of
chronic illnesses and PU (Jaul, Barron, Rosenzwig, Menczel,
2018). Besides, musculoskeletal disorders, neurodegenerative
disorders, and common conditions of malnutrition, anemia, and
infectious disease prevent the healing of wounds and result in
concurrent infections that cause PU. It is also inevitable for
elders with incontinence, hospitalization, and polypharmacy
increase incidences of PU. It thus becomes important that
people who care for the elders and the elders themselves closely
monitor risks and work against them for the better health of the
people. it is important that using chronic participants could
expose a lot of data on the prevalence of PU and help prevent it.
Ethical Considerations
In the first study by Rondinelli et al. (2018), there was a
mutually exclusive agreement that sought approval from KP
Northern California and Southern California Institutional
Review Board for the safeguarding of the participants by
checking braden scale during admissions and protecting,
repositioning patients every 2 hours and protecting the bony
areas of at risk patients with ABD pads. On the other hand, in
Jaul, Barron, Rosenzwig, Menczel (2018) there is no ethical
consideration.
22. References
Jaul, E., Barron, J., Rosenzwig, J.P., Menczel, J. (2018). An
overview of co-morbidities and the development of pressure
ulcers among older adults. BMC Geriatrics, 18, 305.
doi:https://doi.org/10.1186/s12877-018-0997-7
Rondinelli, J., Zuniga, S., Kipnis, P., Kawar, L.N., Liu, v. &
Escobar, G.J. (2018). Hospital-Acquired Pressure Injury Risk-
Adjusted Comparisons in an Integrated Healthcare Delivery
System. Nurs Res., 67(1), 16-25.
doi:10.1097/NNR.0000000000000258