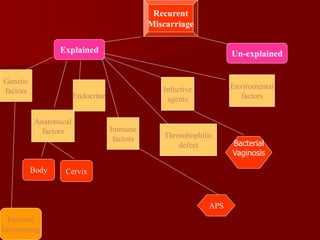
This document summarizes information about recurrent pregnancy loss from Dr. Narendra Gupta of Vivekanand Hospital and Fertility Center in Jaipur, India. It defines recurrent pregnancy loss as 3 or more consecutive spontaneous losses and discusses the psychological impact. It outlines the clinical approach, investigations, and etiological factors that should be considered in evaluating recurrent loss. These include anatomical, endocrine, infectious, immune, thrombophilic, genetic, and unexplained causes. Specific diagnostic tests and treatment approaches are described for several of these factors.






![Infections
TORCH (toxoplasmosis rubella, cytomegalovirus
and herpes simplex virus), other [congenital
syphilis and viruses], screening is unhelpful in the
investigation of recurrent miscarriage.
For an infective agent to be implicated in the
aetiology of repeated pregnancy loss, it must be
capable of persisting in the genital tract and
avoiding detection or must cause insufficient
symptoms to disturb the women. Toxoplasmosis,
rubella, cytomegalovirus, herpes and Listeria
infections do not fulfill these criteria and routine
TORCH screening should be abandoned.](https://image.slidesharecdn.com/recurrentpregnancyloss-230806110705-19a8c418/85/Recurrent-pregnancy-loss-pptx-37-320.jpg)























































![PERI-PROSTHETIC FRACTURE NAIL-PLATE CONSTRUCT [NPC].pptx](https://cdn.slidesharecdn.com/ss_thumbnails/drarunkumardrmohamedashrafperiprostheticfrasturenail-plateconstructnpc-260209164459-7e9d15a1-thumbnail.jpg?width=640&height=640&fit=bounds)













![ONFH[AVN HIP] -TRIPLE REGIME -A NOVAL SURGICAL CONCEPT .pptx](https://cdn.slidesharecdn.com/ss_thumbnails/onfhavnhip2026koaconcalicutdrgokuldevdrmashraf-260210064517-213ec005-thumbnail.jpg?width=640&height=640&fit=bounds)



