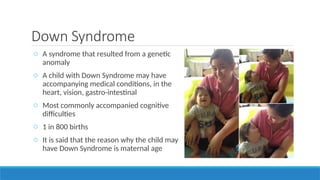
The document presents a comprehensive overview of recognizing and addressing various developmental disabilities in children, including symptoms, diagnosis, and intervention strategies. It covers conditions such as Down syndrome, ADHD, autism spectrum disorder, cerebral palsy, and learning disabilities, emphasizing the importance of early detection and collaborative support from families, schools, and therapists. Practical recommendations for interventions and support systems are also discussed to enhance outcomes for affected children.