Downloaded 24 times
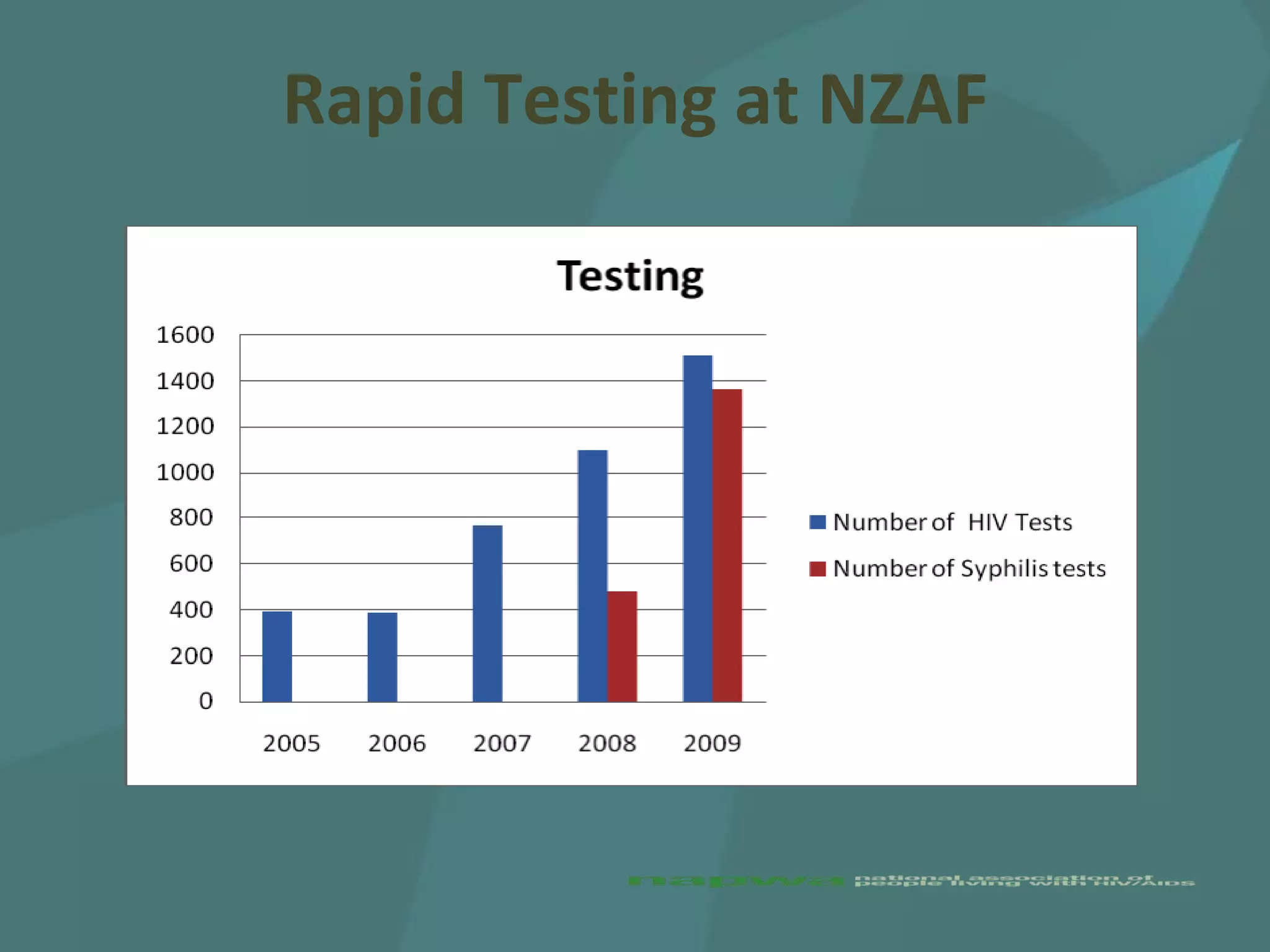
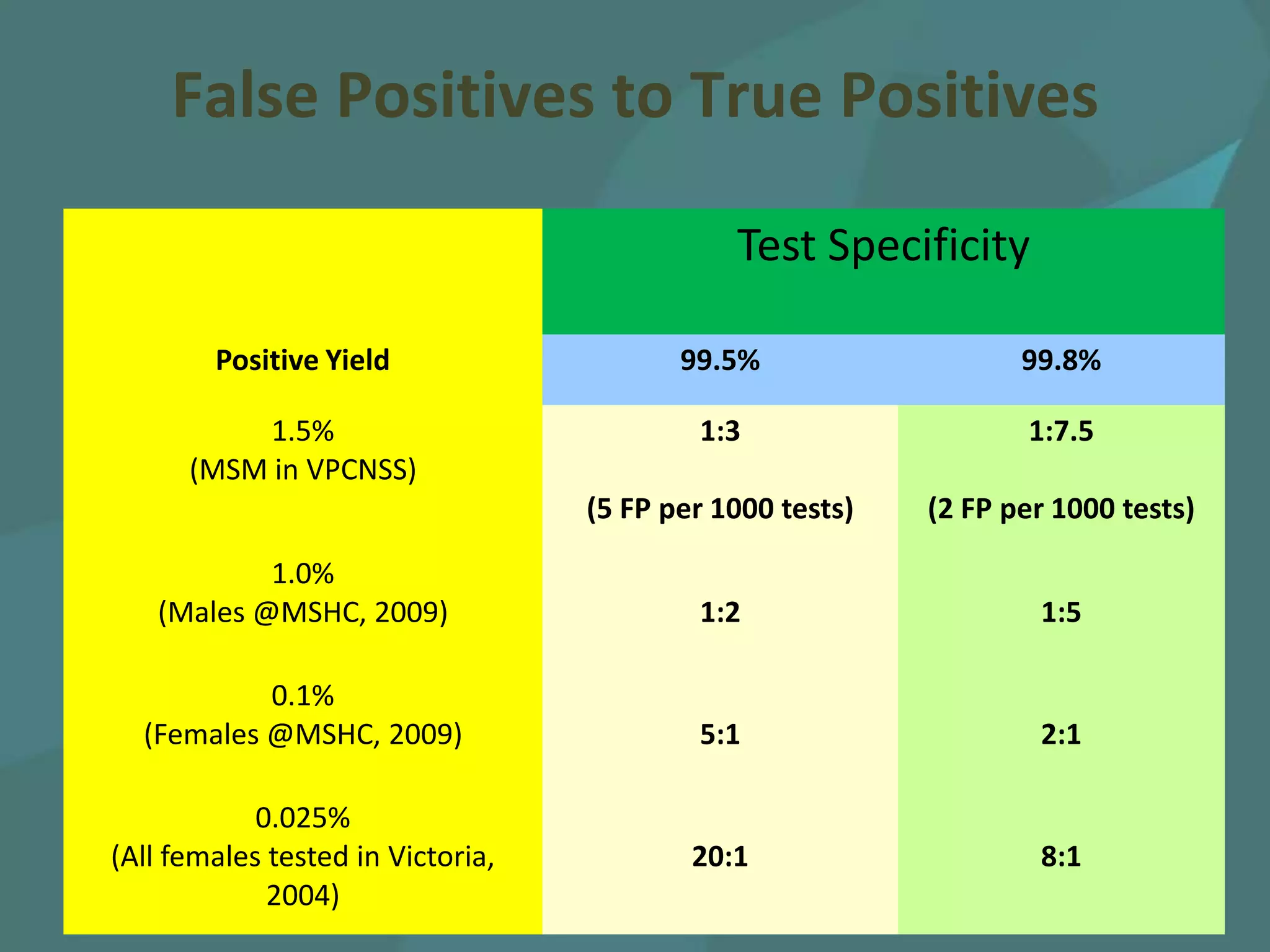




The document discusses the need to scale up rapid HIV testing in order to meet UNPD targets and increase testing coverage, as current testing rates among at-risk groups like MSM are low. It reviews evidence that rapid HIV testing can increase testing rates and yield higher proportions of undiagnosed cases. The document also examines issues around introducing rapid HIV testing services and the policy changes needed to support expanded access to rapid testing.