1.Introduction to theDental Pulp
2.Afferent Pain Pathway
3.Diagnostic Method
• Case History
• Clinical Examination
• Swelling & Pain Evaluation
4.Classification of Pulpal Conditions
5.Endo-Perio Diagnostic Considerations
6.Tests for Cracked Tooth
7.Pulp Testing Techniques
• Thermal Tests
• Electric Pulp Test (EPT)
• Limitations of Sensibility Tests
8.Supplemental Tests
• Test Cavity
• Anesthetic Test
9.Vitality-Based Testing
• Laser Doppler Flowmetry (LDF)
• Pulse Oximetry
• Emerging Technologies
10.Diagnostic Flowchart
11.Summary & Clinical
Implications
12.References
CONTENTS
3.
DENTAL PULP
• ThePulp is a soft mesenchymal connective tissue that
occupies pulp cavity in the central part of the teeth.
4.
‘‘The pulp livesfor the dentin and the dentin
lives by the grace of the pulp.
Few marriages in nature are marked by a
greater affinity.’’Alfred L. Ogilvie
Average
intrapulpal
pressure =10mm
Hg
13 mm in
reversible
35+ mm Hg
irreversible
5.
Nerve Fibers inDental Pulp and
Their Diagnostic Significance
6.
1. Myelinated, fast-conducting
2.Located at the pulp–dentin border, especially in the
coronal pulp
3. Respond to cold stimuli and EPT
4. Responsible for sharp, localized pain
5. Activated early in inflammation
Ingle JI et al. Ingle’s Endodontics. 6th ed.
Hargreaves KM, Berman LH. Pathways of the Pulp. 11th ed.
Types of Nerve Fibers
Aδ fibers
7.
•Unmyelinated, slow-conducting
•Located inthe core of the pulp
•Respond to heat and intense stimuli
•Responsible for dull, lingering pain
•Activated in advanced pulpal inflammation
C fibers
Ingle JI et al. Ingle’s Endodontics. 6th ed.
Hargreaves KM, Berman LH. Pathways of the Pulp. 11th ed.
8.
•Aβ fibers (lesscommon)
•Involved in mechanoreception
•May play a role in pressure sensitivity
Aβ fibers
Ingle JI et al. Ingle’s Endodontics. 6th ed.
Hargreaves KM, Berman LH. Pathways of the Pulp. 11th ed.
9.
•Regulate pulpal bloodflow
•Indirectly influence vitality by modulating vascular
tone
Sympathetic efferent fibers
Ingle JI et al. Ingle’s Endodontics. 6th ed.
Hargreaves KM, Berman LH. Pathways of the Pulp. 11th ed.
10.
AFFERENT PAIN PATHWAY
Impulsefrom
A delta or C
fibres
Plexus of
Raschkow
Nerve trunk
in central
zone of pulp
Apical
foramen exit
Division of
trigeminal
nerve
Pons Thalamus
Cortex
interprets as
pain
11.
•Cold test &EPT: Stimulate Aδ fibers → useful in early
pulpitis
•Heat test: May stimulate C fibers → indicates deeper
inflammation
•Vitality tests (e.g., pulse oximetry): Do not rely on nerve
fibers → assess vascular status directly
•False negatives may occur in immature teeth where Aδ
fibers are underdeveloped
Dimitriu B et al. Acta Sci Med Sci. 2024;8(3):171–5.
Clinical Relevance in Vitality Testing
12.
Temperature
Change
Pulpal Effect ClinicalInsight
↑5.5°C (≈42.5°C)
Risk of irreversible
pulpitis
Seen in 15–40% of
cases (Zach &
Cohen)
↑11°C
Likely pulpal
necrosis
Irreversible damage
confirmed
histologically
↓<21°C
Cold-induced
vasoconstriction,
discomfort
Transient ischemia
may occur in
sensitive teeth
Thermal Thresholds & Pulpal Injury
Baseline pulp temperature: ~34-35 °C. Even small thermal
increases during restorative procedures can endanger pulp
vitality.
Zach L, Cohen G. Pulp response to externally applied heat. J Dent Res. 1965;44(6):1246–1259.
13.
Diagnosis:
‘The art andscience
of detecting
deviations from
health and the cause
and
nature thereof’
HISTORY OF PRESENTILLNESS
• Duration
• Mode of onset
• Progression
• Severity
• Nature
• Aggravating/relieving factors
• Postural variation
• Any medications/treatment
received for the same
Elaboration of
complaint(pain)
19.
PAIN
• Most commoncomplaint that leads to dental
treatment
• According to intensity
Mild pain
• Controlled
by simple
analgesics
Moderate
pain
• Controlled
with narcotic
analgesics
Severe pain
• Cannot
controlled
with
analgesics
• Require
elimination
of cause
20.
According to nature
•Pricking/piercing
• Throbbing
• Lancinating
• Aching
• Dull, boring, gnawing
Localization of pain
• Localised when
patient can point to a
specific tooth or site
• Sharp , piercing and
lancinating pain in a
tooth responds to
cold and is easy to
localize
• Dull, boring pain is
diffuse and responds
abnormally to heat
than to cold is
difficult to localize.
21.
ACCORDING TO DURATION
•Pain of short duration & separated
by wholly pain free period
Intermittent
• Pain of longer duration
Continuous
• Two or more similar episodes of
pain
Recurrent
Periodic
• Characterized by regularly
recurring episode
22.
ACCORDING TO ONSET
•Pain occurs without
being provoked
Spontaneous
• Provocation causes
painful sensation
Induced
• When evoked
response is out of
proportion to the
stimulus
Triggered
23.
SWELLING
Anatomical location(site)
Duration
Mode of onset
Symptoms
Progress of swelling
Associated features
Secondary changes
Impairment of function
Recurrence of swelling
24.
PAST MEDICAL HISTORY
-Anemia
-Bleedingdisorders
-Cardio respiratory disorders
-Drug treatment and allergies
-Endocrine disorders
-Fits and faints
-Gastrointestinal disorders
-Hospital admissions and surgeries
-Infections
-Jaundice and liver diseases
-Kidney disease
Checklist by Scully & Cawson
INTRAORAL EXAMINATION
Soft tissueexamination:
Swelling/ fistula
Crown discoloration: non vital
pulp
Deep carious lesions/ fractures:
visual examination & probing
29.
PERCUSSION
•Percussion testing evaluatesthe periapical status of a
tooth, not the pulp directly.
•It helps detect inflammation of the periodontal ligament
(PDL), which may result from pulpal necrosis or periapical
pathology.
30.
Step Description
Instrument
Handle ofa mouth mirror or
blunt instrument
Direction
Vertical (occlusal) and
horizontal (buccal-lingual)
tapping
Comparison
Always compare with
adjacent and contralateral
teeth
Patient Feedback
Ask patient to report pain,
tenderness, or discomfort
🧪 How It’s Performed
31.
Response Clinical Implication
Nopain
Normal PDL and likely
healthy pulp
Mild discomfort
Possible early inflammation
or occlusal trauma
Sharp pain on percussion
Suggests periapical
inflammation, often due to
pulpal necrosis
Pain on lateral percussion
May indicate cracked tooth
syndrome or periodontal
involvement
🧠 Interpretation of Responses
1.Hargreaves KM, Berman LH. Cohen’s Pathways of the Pulp. 11th ed. St. Louis: Elsevier; 2016. p. 92–95.
2.Torabinejad M, Walton RE. Endodontics: Principles and Practice. 5th ed. Saunders; 2014. p. 108–110.
2.Animated Teeth. Root canal testing – percussion, thermal, and electric pulp tests [Internet]. 2023 [cited 2025 Jul 4].
32.
PALPATION
Purpose
Palpation assessesthe periapical and surrounding soft
tissues for signs of inflammation, infection, or swelling.
It does not test pulp vitality directly, but helps identify
periapical pathology that may result from pulpal necrosis.
33.
Step Description
Finger Pressure
Usegloved index finger to
apply gentle pressure over the
facial/buccal mucosa near
the apex of the suspect tooth
Comparison
Always compare with
contralateral and adjacent
teeth
Observation
Look for tenderness,
swelling, induration, or
fluctuation
Patient Feedback
Ask patient to report pain,
pressure, or discomfort
🧪 How It’s Performed
1.Hargreaves KM, Berman LH. Cohen’s Pathways of the Pulp. 11th ed. St. Louis: Elsevier; 2016. p. 92–95.
34.
⚠️ Note: Palpationfindings must be correlated with
percussion, thermal/electric tests, and radiographs
for accurate diagnosis.
Interpretation of Findings
Finding Clinical Implication
No tenderness Normal periapical tissues
Localized tenderness
Suggests periapical
inflammation (e.g., apical
periodontitis)
Swelling or fluctuation
May indicate acute abscess
or chronic infection
Induration
Possible chronic
inflammatory response
35.
MOBILITY
• Purpose
• Mobilitytesting evaluates the integrity of the periodontal
ligament (PDL) and alveolar bone support.
• While it does not directly assess pulp vitality, increased
mobility may indicate periapical inflammation, trauma, or
periodontal disease—all of which can affect pulp health.
36.
Step Description
Instrument
Use twoblunt instruments
(e.g., mirror handle + probe)
Direction
Apply gentle pressure
buccolingually (horizontal)
and vertically (optional)
Comparison
Always compare with
adjacent and contralateral
teeth
Grading
Use Miller’s Classification
to quantify mobility
How It’s Performed
37.
Grade Description
Grade 0
Normalphysiological
mobility
Grade I Slight mobility
Grade II
Moderate mobility (>1 mm)
in horizontal direction
Grade III
Severe mobility (>1 mm
horizontal + vertical
depressibility into socket)
Miller’s Classification of Tooth
Mobility
1.Hargreaves KM, Berman LH. Cohen’s Pathways of the Pulp. 11th ed. St. Louis: Elsevier; 2016. p. 92–95.
2.Torabinejad M, Walton RE. Endodontics: Principles and Practice. 5th ed. Saunders; 2014. p. 108–110.
38.
PERIODONTAL
PROBING
• Purpose
• Periodontalprobing assesses the depth of the gingival
sulcus or periodontal pocket around a tooth.
• While it does not directly test pulp vitality, it helps identify
periodontal-endodontic lesions, vertical root fractures, or
isolated deep pockets that may indicate pulpal pathology.
39.
Step Description
Instrument
Use acalibrated
periodontal probe (e.g.,
UNC-15, Williams)
Sites
Probe six points per tooth
(mesiobuccal, midbuccal,
distobuccal, and lingual
equivalents)
Technique
Insert probe gently into
sulcus, parallel to root
surface, using light pressure
Measurement
Record probing depth in
millimeters
How It’s Performed
40.
Probing Depth ClinicalInterpretation
1–3 mm Healthy periodontium
4–5 mm
Early periodontitis or
gingival inflammation
≥6 mm
Moderate to severe
periodontitis
Isolated deep pocket
May indicate vertical root
fracture or endo-perio
lesion
Interpretation of Findings
41.
Finding Possible Implication
Generalizeddeep pockets
Periodontal origin; pulp may
still be vital
Isolated narrow deep pocket
May suggest vertical root
fracture or draining sinus
from necrotic pulp
Deep pocket + nonvital pulp
Suggests primary
endodontic lesion with
secondary periodontal
involvement
Deep pocket + vital pulp
Likely primary periodontal
lesion
Relevance to Pulp Vitality
1.Hargreaves KM, Berman LH. Cohen’s Pathways of the Pulp. 11th ed. St. Louis: Elsevier; 2016. p. 92–95.
2.Torabinejad M, Walton RE. Endodontics: Principles and Practice. 5th ed. Saunders; 2014. p. 108–110.
42.
TEST CAVITY
•A testcavity involves drilling into enamel and dentin
without local anesthesia to assess the presence of vital pulp
tissue based on the patient's pain response.
•It is used when cold, heat, electric pulp tests, and
radiographs fail to provide a definitive diagnosis.
43.
Step Description
Isolation
Tooth isisolated and dried
(rubber dam optional)
No Anesthesia
Performed without local
anesthesia to preserve sensory
feedback
Access with High-Speed Bur
A small cavity is prepared
through enamel into dentin
Patient Feedback
Patient is asked to report any
pain or sensitivity during
drilling
Response Interpretation
Pain = vital pulp; No pain =
possible necrosis
Restoration
If pulp is vital, cavity is
restored immediately
🧪 Procedure Overview
44.
Clinical Interpretation
Response Implication
Sharppain in dentin Vital pulp present
No response in dentin
Suggests necrotic or non-
vital pulp
Delayed response
May indicate partial
necrosis or calcification
45.
🚫 Limitations &Ethical Considerations
•Invasive: Irreversibly removes tooth structure.
•Anxiety-inducing: May cause distress without anesthesia.
•Rarely used: Reserved for exceptional diagnostic
dilemmas.
•Not standardized: Lacks reproducibility and is not
evidence-based compared to modern vitality tests.
⚠️Note: In multi-rooted teeth, one canal may still be vital—
so a negative response doesn’t always confirm total necrosis.
46.
ANESTHETIC TEST
Purpose
• Tolocalize the offending tooth when conventional tests
(cold, heat, EPT) are inconclusive.
• Particularly useful in posterior teeth, where pain may be
referred across arches or quadrants.
47.
Step Description
Baseline Assessment
Recordpatient’s pain history
and suspected quadrant
Local Anesthesia
Administered
Infiltration or nerve block
(e.g., IAN block for
mandibular teeth)
Observe Pain Response
If pain disappears → source
lies within anesthetized area
Sequential Testing
If pain persists, anesthetize
adjacent quadrant or arch
Final Confirmation
Once pain is eliminated,
isolate and test individual
teeth in that region
How It’s Performed
48.
🧠 Clinical Interpretation
ObservationImplication
Pain eliminated after
anesthesia
Offending tooth is within
anesthetized region (likely
necrotic or inflamed pulp)
Pain persists
Source lies outside
anesthetized area; consider
referred pain or non-
odontogenic origin
49.
🔍 Definition
A crackedtooth is an incomplete fracture that begins in
the crown and may extend subgingivally, often in a
mesiodistal direction. It may involve enamel, dentin, and
potentially the pulp.
Cracked Tooth: Endodontic
Perspective
50.
Crack Depth PulpStatus
Confined to enamel Pulp usually unaffected
Into dentin, not reaching
pulp
May cause reversible
pulpitis
Extending into pulp
chamber
Often leads to irreversible
pulpitis or necrosis
Extending into root
Poor prognosis; may
require extraction
🧠 Pulpal Implications
51.
Test Purpose KeyIndicators
Bite Test (Tooth
Slooth™ /
FracFinder)
Identifies pain on
biting or release of
pressure
Sharp pain on
release = classic
sign of cracked cusp
or cracked tooth
Transillumination
Uses fiber-optic
light to reveal crack
lines
Crack blocks light
transmission;
appears as a dark
line
Diagnostic Tests for Cracked Tooth
52.
Staining with Dyes
Methyleneblue or
gentian violet
highlights fracture
lines
Crack absorbs dye
and becomes visible
under magnification
Tactile Test
Explorer tip catches
on crack line
“Catch” or drag
sensation when
moving explorer
across suspected
area
53.
Removal of
Restoration
Exposes hidden
cracksbeneath
restorations
Visual confirmation
of fracture line on
cavity floor or walls
Periodontal
Probing
Detects isolated deep
pockets from root
fractures
Narrow, deep pocket
adjacent to crack =
possible vertical root
fracture
Radiographs
(Multiple Angles)
May show widened
PDL or radiolucency
if crack extends
apically
Limited utility unless
crack is buccolingual
or causes periapical
changes
54.
CBCT Imaging
3D visualizationof
root and crown
structures
May detect vertical
root fractures or
deep cracks not
visible on 2D
radiographs
Microscopic
Examination
Dental operating
microscope
enhances crack
detection
Useful for
identifying craze
lines vs true cracks
55.
️
🛠️Management Strategies
Crack TypeTreatment Approach
Superficial enamel crack
Monitor or smoothen; no
intervention needed
Cracked cusp
Remove cusp + restore with
onlay or crown
Cracked tooth (into pulp)
Endodontic therapy + full-
coverage restoration
Vertical root fracture
Often non-restorable;
extraction recommended
Vital pulp with crack
Consider vital pulp therapy
(e.g., Biodentine™ pulpotomy)
if inflammation is limited
56.
•Pain on release(not just on biting) is a hallmark of cracked
tooth syndrome.
•Always test each cusp individually using a bite stick to
localize the crack.
•Combine tests for higher diagnostic accuracy—e.g.,
transillumination + staining + bite test.
1.Markose A. Crack tooth syndrome: Diagnosis and management [Internet]. IOSR J Dent Med Sci. 2020 [cited 2025
Jul 4];19(10):4–9.
57.
DYE STAINING
Purpose
•Enhances visualizationof enamel and dentinal
cracks that may not be visible to the naked eye.
•Helps differentiate between craze lines,
structural cracks, and vertical root fractures.
•Aids in treatment planning, patient education,
and documentation for insurance or referral.
58.
Dye Color Properties
MethyleneBlue Deep blue
High contrast, pools
in cracks, excellent
for photography and
documentation
Gentian Violet Purple
Similar to
methylene blue; less
commonly used
Caries Indicator
Dyes
Pink/Red
Less effective for
cracks; designed for
carious dentin
detection
🧬 Commonly Used Dyes
59.
1.Clean the tooth:Use pumice slurry or air polishing to
remove plaque and debris.
2.Dry the surface: Isolate and gently air-dry the tooth.
3.Apply dye: Use a microbrush to apply methylene blue to the
suspected area.
4.Wait 10–15 seconds: Allow dye to penetrate microfractures.
5.Rinse and dry: Gently rinse and air-dry to reveal stained
crack lines.
6.Examine under magnification: Use a dental operating
microscope (DOM) or high-power loupes.
🧰 Clinical Protocol
60.
🧠 Tip: Dyestaining is especially useful after removing
restorations, as many cracks originate beneath amalgams or
composites.
1.Markose A. Crack tooth syndrome: Diagnosis and management [Internet]. IOSR J Dent Med Sci. 2020 [cited
2025 Jul 4];19(10):4–9.
61.
•May overstain plaqueor sodium hypochlorite-treated dentin.
•Cannot differentiate between active vs. inactive cracks.
•May mask subtle color changes when used with
transillumination.
Limitations
1.Markose A. Crack tooth syndrome: Diagnosis and management [Internet]. IOSR J Dent Med Sci. 2020 [cited
2025 Jul 4];19(10):4–9.
62.
🔍 Purpose
•To localizepain caused by incomplete fractures in enamel
or dentin.
•Especially useful in posterior teeth where cracks are often
not visible radiographically.
Bite Test for Cracked Tooth
Detection
63.
🧪 How It’sPerformed
Step Description
Instrument
Use a Tooth Slooth™,
FracFinder™, cotton roll, or
orange wood stick
Application
Place the device on individual
cusps, one at a time
Patient Action
Instruct patient to bite down
and release
Observation
Note any sharp pain on biting
or release—especially on
release
64.
🧠 Pain onrelease is a hallmark of cracked tooth syndrome
due to separation and rebound of fractured segments.
Response Clinical Implication
Pain on biting May indicate fractured cusp
Pain on release
Suggests incomplete crack
extending into dentin
No pain
Likely no crack or not in tested
cusp
Interpretation of Results
65.
Why It Works
•Bitingseparates the crack, stimulating A-delta fibers in
dentin.
•Releasing pressure causes rebound movement, triggering
sharp pain.
1.Markose A. Crack tooth syndrome: Diagnosis and management [Internet]. IOSR J
Dent Med Sci. 2020 [cited 2025 Jul 4];19(10):4–9.
66.
BITE TEST
Interpretation
Pain onbiting: Symptomatic apical
periodontitis
Pain on release of force: Cracked
tooth
•Pitt Ford. Endodontics: Problem Solving
67.
Condition Clinical FeaturesTest Response
Normal Pulp
No symptoms;
responds normally
to stimuli
Cold/EPT:
Positive, brief pain
Reversible
Pulpitis
Sharp, transient
pain to cold; no
spontaneous pain
Cold: Positive,
non-lingering
Symptomatic
Irreversible
Pulpitis
Lingering/
spontaneous pain;
sensitive to
cold/heat
Cold: Lingering;
EPT: Positive
Classification of Pulpal Conditions
•Berman LH, Hargreaves KM. Pathways of the Pulp, 10th ed.
•Ingle JI et al. Endodontics, 6th ed.
•Jafarzadeh H, Abbott PV. Int Endod J. 2010;43(9):738–762.
Why It's Important
Accuratepulp vitality testing helps determine the origin of
lesions—whether primarily endodontic, periodontal, or a true
combined lesion—guiding appropriate treatment.
Endo-Perio Lesion Identification
& Pulp Vitality Testing
71.
Lesion Type
Vitality Test
Result
Interpretation
PrimaryEndodontic
Lesion
Pulp test: Non-
vital
Pulpal infection
drains via
periodontal
structures
Primary Periodontal
Lesion
Pulp test: Vital
Periodontal
inflammation
only; pulp
remains
unaffected
Vitality Test Outcomes & Diagnosis
72.
Lesion Type
Vitality Test
Result
Interpretation
PrimaryEndo with
Secondary Perio
Pulp test: Non-vital
Pulpal origin
spreads to
periodontium
Primary Perio with
Secondary Endo
Pulp: Initially vital,
progresses to non-
vital
Chronic
periodontitis affects
pulp via
lateral/accessory
canals
True Combined
Lesion
Pulp test: Non-vital
Simultaneous
pulpal &
periodontal
involvement
🧪 Vitality Test Outcomes & Diagnosis
73.
•Vital pulp +isolated deep pocket = primary periodontal
•Non-vital pulp + narrow pocket = primary endodontic
•Tracing sinus tract to apex = endodontic origin
•Always correlate clinical, radiographic, and vitality test
findings
1.Keerthika R, Nivedhitha MS. J Res Med Dent Sci. 2021;9(2):140–145.
2.Tambe V et al. IJRTI. 2022; IJRTI2209089
3.Jafarzadeh H, Abbott PV. Int Endod J. 2010;43(9):738–762.
4.Yoon SY et al. J Endod. 2010;36(3):375–8.
Diagnostic Pearls
74.
IMPORTANCE OF PULPTESTING
Ideal technique Attributes(chambers,1982): non invasive,
painless, standardized, reproducible, reliable, inexpensive,
easily completed & objective
Goal: Differentiate between vital,inflamed, or necrotic pulp
Pulp sensibility
tests
• Thermal tests
• Electric pulp
tests
• Test cavity
Pulp vitality
tests
• Laser doppler
flowmetry
• Pulse oximetry
• Tooth
temperature
Measurement
75.
Recent studies haveshown that blood circulation and not
innervations is the most accurate determinant in assessing pulp
vitality as it provides an objective differentiation between
necrotic and vital pulp tissue.
Tomer AK, Raina AA, Ayub F, Bhatt M. Recent advances in pulp vitality testing: A review. Int. J. Appl. Dent. Sci.
2019;5:8-12.
76.
Introduction
What is PulpVitality?
•Refers to the vascular integrity of the dental pulp, not
merely nerve response
•Essential for maintaining pulpal health, reparative
capacity, and immune defense
Kumar S et al. Diagnostic Accuracy of Pulp Vitality Tests: A Systematic Review.
Int J Environ Res Public Health. 2022;19(15):9599.
77.
Sensitivity is definedas "the ability to respond to a
stimulus"
Sensibility indicates neural response (A delta and C fibers)
Whereas vitality is defined as "the capacity to live, grow, or
develop.“
Reference: Ingle JI et al. Ingle’s Endodontics, 7th ed.
78.
Sensitivity: Probability ofcorrectly identifying a vital pulp.
Specificity: Probability of correctly identifying a necrotic
pulp.
PPV/NPV: Reflect the predictive power of tests in real-life
conditions.
Kumar S et al. Diagnostic Accuracy of Pulp Vitality Tests: A Systematic Review. Int J Environ Res
Public Health. 2022;19(15):9599.
Diagnostic Parameters
Definitions:
79.
VALUE OF DIAGNOSTICTESTS
Negative predictive value: The
probability that a tooth with a negative
test result is actually free from the
disease
Heat: relatively high sensibility; but least
accurate being the least specific
Cold test: more accurate than EPT
Positive predictive value: The
probability that a positive test result
actually represents a disease
positive tooth
80.
🟢 Sensitivity
Vital pulp→ Test applied → True Positive result
•Meaning: Detects vital pulp accurately when it is truly vital.
•Clinical relevance: Avoids unnecessary treatment of healthy
pulps.
🔴 Specificity
Non-vital pulp → Test applied → True Negative result
•Meaning: Identifies non-vital pulp correctly when vitality is
absent.
•Clinical relevance: Prevents overlooking necrotic tissues.
81.
🔁 High sensitivity+ specificity = Increased diagnostic
confidence
Tests like pulse oximetry and laser Doppler flowmetry excel in
both aspects.
82.
Test Sensitivity Specificity
Subjective/
Objective
ColdTest Moderate High Subjective
Electric
Pulp Test
Moderate Moderate Subjective
Pulse
Oximetry
High High Objective
Laser
Doppler
Flowmetry
High High Objective
Comparative Accuracy of Tests
Takeaway: Vitality tests are superior in accuracy and reliability
83.
The ideal pulptest should provide a
* Simple
* Objective
* Standardized
* Reproducible
* Non-painful
* Non-injurious
* Accurate
* Inexpensive way of assessing the condition of the
pulp tissue.
84.
Sources:
AAE (American Associationof Endodontists): Advocates
vitality assessment for diagnosis and prognosis.
ESE (European Society of Endodontology): Stresses
combined use of clinical tests.
BES (British Endodontic Society): Emphasizes vitality
testing in trauma cases.
Clinical Guidelines
American Association of Endodontists. AAE Position Statement onVital Pulp
Therapy. Chicago:AAE; 2021
85.
Pediatric: Incomplete apexformation—pulse oximetry
preferred.
Geriatric: Pulp calcifications—vitality tests more reliable.
Trauma: Sensibility often unreliable initially.
Scenarios:
86.
DEFINITIONS
PULP SENSITIVITY TEST
Adiagnostic procedure to determine pulpal status; can be
performed with electrical, mechanical or thermal
methodologies to assess the pulp's response to stimuli.
PULP VITALITY TEST
A diagnostic procedure to determine pulpal status by the
assessment of blood supply to the tooth.
87.
USES OF PULPTESTING
Diagnosis of Pulpal Pathology
•Helps differentiate between reversible and irreversible
pulpitis, or pulp necrosis.
•Cold and EPT tests are commonly used to assess neural
response.
Gopikrishna V, Pradeep G, Venkateshbabu N. Assessment of pulp vitality: A review. Int J Paediatr Dent.
2009;19(1):3–15.
88.
Assessment After DentalTrauma
•Vitality tests (e.g., pulse oximetry) are preferred in
traumatized teeth where nerve response may be temporarily
lost.
European Society of Endodontology. Position statement: Management of deep
caries and the exposed pulp. Int Endod J. 2019;52(7):923–34.
89.
Treatment Planning forEndodontics
•Determines whether root canal therapy or vital pulp therapy
is indicated.
American Association of Endodontists. AAE Position Statement on Vital Pulp Therapy. 2021
90.
Monitoring Pulpal StatusOver Time
•Useful in follow-up of teeth with deep restorations, trauma,
or orthodontic movement.
•Reference: Abbott PV. Dental pulp testing: A review. Int J Dent.
2009;2009:365785.
91.
Differentiating Odontogenic vs.Non-Odontogenic Pain
•Helps localize the source of pain and rule out referred pain
from non-dental origins.
•Reference: Tomer AK, Raina AA, Ayub FB, Bhatt M. Recent advances in pulp vitality testing: A
review. Int J Appl Dent Sci. 2019;5(3):8–12.
92.
Pre-Prosthodontic Evaluation
•Ensures pulpalhealth before placing crowns or bridges to
avoid post-treatment complications.
Dimitriu B, âncu AM, Nistor C, Amza O. Dental pulp assessment – The first step towards an accurate
Ț
diagnostic in endodontics. Acta Sci Med Sci. 2024;8(3):171–5.
93.
• To diagnoseoral pain whether it is of pulpal or
periodontal origin or because of other reason.
• To assess vitality of traumatized teeth
• To check the status of tooth especially which has
past history of pulp capping or deep restoration.
94.
•Differentiates between reversiblepulpitis, irreversible
pulpitis, and pulp necrosis
•Guides treatment planning: pulpotomy, pulpectomy, RCT,
or monitoring.
Why Accurate Testing Matters
Kayalvizhi G & Subramaniyan B. J Oral Health Comm Dent. 2011;5(1):12–14
95.
Cold, heat, andEPT rely on subjective patient response May
yield false positives/negatives in trauma, immature teeth,
calcifications (Kayalvizhi & Subramaniyan, 2011)
Kayalvizhi G & Subramaniyan B. J Oral Health Comm Dent. 2011;5(1):12–14
Limitations of Traditional Sensibility Tests
96.
Pulse oximetry: measuresoxygen saturation in pulpal
vessels
Laser Doppler Flowmetry: detects microvascular blood
flow (Gopikrishna et al., 2009; Tomer et al., 2019)
•Gopikrishna V et al. J Endod. 2007;33(4):411–414
•Tomer AK et al. Int J Appl Dent Sci. 2019;5(3):8–12
Modern Vitality-Based Tools
Classification of PulpTesting Methods
I. Sensibility Tests
Assess neural response (Aδ and C fibers) 🧠
Subjective – depend on patient perception
TestType Examples Key Features
ThermalTests
Cold (CO snow,
₂
refrigerant spray)
<br> Heat (Gutta-
percha, hot water)
Quick, widely
used, but prone to
false results
Electric Pulp
Test (EPT)
Low current
stimulation
Useful in mature
teeth; not reliable
in trauma or
immature apex
99.
Limitation: May givefalse positives/negatives in
calcified canals, trauma, or young permanent teeth
•Gopikrishna V et al. J Endod. 2007;33(4):411–414.
•Petersson et al., J Endod. 1999;25(1):5–8
100.
II. Vitality Tests
Assessvascular supply – true indicator of pulp health 🩸
Objective – independent of patient response
Test Type Principle Advantages
Pulse Oximetry
Measures oxygen
saturation
Non-invasive,
reproducible,
reliable
Laser Doppler
Flowmetry (LDF)
Detects
microvascular
blood flow
High sensitivity,
especially in trauma
cases
Transmitted Laser
Light (TLL)
Measures light
absorption by blood
Still under research;
promising for
future use
101.
Clinical Tip: Usein trauma, immature teeth, or
when sensibility tests are inconclusive
Reference: Gopikrishna et al., 2009; Tomer et al., 2019
102.
Thermal Testing inPulp Diagnosis
Thermal tests assess the sensory response of Aδ fibers in the
pulp to temperature changes. They are quick, non-invasive,
and widely used in clinical practice.
Test Stimulus Application
Cold Test
CO snow,
₂
refrigerant spray
(Endo-Ice), ice
sticks
Most reliable;
stimulates Aδ fibers
Heat Test
Heated gutta-
percha, hot water,
frictional heat
Used when cold test
is inconclusive
Types of Thermal Tests
103.
Note: Cold testis more reliable than heat test for detecting
pulp necrosis
Petersson et al., J Endod. 1999;25(1):5–8
104.
The cold testis a pulp sensibility test that evaluates
the neural response of the pulp to cold stimuli,
primarily targeting A-delta fibers. It is widely used
due to its simplicity, reliability, and diagnostic
value.
cold test
Kwan SC. Spotlight on pulp testing. Endodontic Spotlight. 2013;2(3):5.
105.
•Cold causes rapidoutward fluid movement in dentinal
tubules (hydrodynamic theory).
•This stimulates A-delta fibers, producing a sharp, localized
pain.
•A normal response is brief and non-lingering.
•A lingering response suggests irreversible pulpitis.
•No response may indicate pulp necrosis, though false
negatives are possible.
🧪 Principle
Property DDM (OldAgent)
TFE (Current
Agent)
Chemical Name
Dichlorodifluorome
thane
1,1,1,2-
Tetrafluoroethane
Refrigerant Code R-12 R-134a
Pulp Testing Use
Cold test agent
(Endo Ice)
Cold test agent
(modern Endo Ice)
Reason for
Discontinuation
Ozone-depleting
substance under
the Montreal
Protocol
Environmentally
safer alternative
Regulatory Status
Banned globally for
most uses since the
1990s
Approved for
medical/dental use
Why DDM (Dichlorodifluoromethane) Was Discontinued
in Endo Ice
1.Kwan SC. Spotlight on pulp testing. Endodontic Spotlight. 2013;2(3):5.
108.
Stimulus Temperature ApplicationMethod
Endo Ice (1,1,1,2-
Tetrafluoroethane)
−26.2°C to −50°C
Cotton pellet soaked
and applied to mid-
facial crown
CO Snow (Dry Ice)
₂ −78.5°C
Compacted into a stick
and applied with
forceps
Ice Stick 0°C
Made from frozen
water in anesthetic
cartridges
Refrigerant Spray −20°C to −50°C
Sprayed on cotton
pellet and applied
Cold Water Bath ~0–4°C
Used under rubber
dam for full-coverage
restorations
Common Cold Stimuli & Techniques
109.
MECHANISM OF COLDTEST
Cold application for more than 15 seconds
+ve
response
Similar to
contralateral
Short sharp pain
that disappears
rapidly on removal
of stimulus
Excruciatingly
painful
response that
lingers even on
stimulus
removal
No
response
Healthy
pulp
Reversible
pulpitis
Irreversible
pulpitis
Non vital
tooth
110.
Response Pulp Status
Sharp,brief pain Normal vitality
Lingering pain after
stimulus
Irreversible pulpitis
No response
Possible necrosis or
calcification
Delayed response
Degenerating pulp or
trauma
Interpretation of Responses
111.
•Sensitivity: ~89%
•Specificity: ~83%
•Mostaccurate among sensibility tests for detecting vital
pulp, especially in anterior teeth.
Diagnostic Accuracy
Decisions in Dentistry. Principles of endodontic diagnosis [Internet]. 2022 [cited 2025 Jul 4]
112.
•Subjective: Depends onpatient perception.
•False negatives: Common in calcified, traumatized, or
immature teeth.
•False positives: May occur due to anxiety or adjacent
tooth conduction.
Decisions in Dentistry. Principles of endodontic diagnosis [Internet]. 2022 [cited 2025 Jul 4]
⚠️Limitations
113.
Parameter
Traditional
Methods
Advanced
Methods
Examples
Endo Ice, DryIce,
Ice Stick, Cold
Water Bath
Calset™ Digital
Cold Tester,
Modified
Tetrafluoroethane
Sprays
Temperature
Control
Unregulated;
manually chilled
materials (~−26°C
to 0°C)
Digitally calibrated
devices (~−50°C)
with precise
temperature and
timing control
Comparison of Traditional and Advanced Cold
Test Methods
1.Adam M. ‘Cold is gold’? The diagnostic accuracy of sensibility and vitality testing techniques [Internet]. Evid Based
Dent. 2022 [cited 2025 Jul 4];23:137.
Clinical Challenges
Difficult in
heavilyrestored
or calcified teeth
Improved
performance in
cases of trauma,
open apex, or
multi-surface
restorations
Interpretation Bias
High; depends
solely on patient
feedback
Reduced with
integrated
multimodal
tools (e.g.,
combining with
Pulse Oximetry
or LDF)
1.Adam M. ‘Cold is gold’? The diagnostic accuracy of sensibility and vitality testing techniques [Internet]. Evid Based
Dent. 2022 [cited 2025 Jul 4];23:137.
116.
Availability
Widely
available, low
cost
Limited clinical
use(research
phase for
some), requires
investment in
newer tech
1.Adam M. ‘Cold is gold’? The diagnostic accuracy of sensibility and vitality testing techniques [Internet]. Evid Based
Dent. 2022 [cited 2025 Jul 4];23:137.
117.
The heat testis a pulp sensibility test that evaluates the
neural response of the pulp to thermal stimuli. It helps
differentiate between vital, inflamed, and necrotic pulps
based on the patient's subjective response.
HEAT TEST
Mousavi et al. (2017): Used heated gutta-percha applied with electric heat carriers in their
comparative study on pulp test accuracy.
118.
•Heat stimulates C-fibersin the pulp, which are associated
with dull, lingering pain.
•A prolonged or exaggerated response may indicate
irreversible pulpitis.
•No response may suggest pulp necrosis, though false
negatives are possible.
Principle
Mousavi et al. (2017): Used heated gutta-percha applied with electric heat carriers in their
comparative study on pulp test accuracy.
119.
Traditional Method Description
Heatedgutta-percha
Applied to the tooth surface
with petroleum jelly as a
separator
Hot water bath
Immersion of the tooth in
warm water
Rubber cup friction
High-speed handpiece
without water to generate
heat
Hot burnisher
Metal instrument heated and
applied to the tooth
Common Techniques
120.
Device/Method Mechanism ClinicalUse
Electric Heat
Carrier
Electrically heated
plugger or
instrument tip (e.g.,
Touch’n Heat)
Delivers controlled
heat to gutta-percha
or directly to tooth
Hot Burnisher
Metal instrument
heated via electric
coil or flame
Applied to tooth
surface to elicit
response
Common Electrical Heat Sources in
Pulp Testing
•Mousavi et al. (2017): Used heated gutta-percha applied with electric heat carriers in their comparative study
on pulp test accuracy.
•Lado et al. (2018): Discussed the importance of standardized stimulus delivery in pulp testing, including
electric heat tools for consistency.
•Modaresi et al. (2013): Evaluated how thermal changes affect electric pulp test responses, emphasizing
the interplay between heat and electrical stimuli.
121.
Device/Method Mechanism ClinicalUse
Electric Heating
Unit
Bench-top devices
with adjustable
temperature settings
Used to heat gutta-
percha or
instruments
Frictional Heat
via Handpiece
High-speed
handpiece without
coolant generates
heat through friction
Indirect electrical
source; used
cautiously
Laser Devices
(e.g., Diode)
Emit focused energy
that converts to heat
at the tissue interface
Experimental use in
thermal pulp testing
123.
Tooth Type HeatTest Accuracy
Anterior 82.6%
Premolar 78.1%
Molar 72.7%
According to a comparative study by Mousavi et al. (2017):
•The heat test showed the highest sensitivity (87.2%) among
thermal and electrical tests for detecting pulp vitality.
•However, specificity was lower, especially in anterior teeth
(63.3%), indicating a higher chance of false positives.
Diagnostic Accuracy
124.
•Subjective: Depends onpatient perception and
communication.
•False positives: May occur in teeth with residual
inflamed pulp tissue.
•Risk of damage: Excessive heat can harm the pulp or
surrounding tissues if not carefully controlled.
Limitations
Response Clinical Implication
Sharppain, subsides
quickly
Normal or reversible
pulpitis
Lingering pain >10 seconds
Suggestive of irreversible
pulpitis
No response
Possible pulp necrosis
(confirm with vitality test)
Interpretation of Responses
📌 Tip: Always compare with adjacent and contralateral
teeth for baseline.
127.
🔹 Principle
•EPT stimulatesAδ nerve fibers in the pulp using a low
electrical current
•A positive response indicates presence of vital sensory
fibers, not necessarily pulp health
•Does not assess vascular supply—so not a true vitality
test (Lado et al., 2018; Bittner, 2018)
Electric Pulp Testing (EPT)
Clinical protocol adapted from Pathways of the Pulp, 12th ed.
128.
ELECTRICAL PULP TESTING
Directstimulation of pulp nerve
fibers
Unreliable: necrotic &
disintegrating pulp tissue leaves
electrolytes in pulp space
Adequate stimulation, appropriate
technique, careful interpretation
AC or DC; Pulsating DC: 5-15ms
best nerve stimulation
Benchtop style digital EPT
Handheld digital style EPT
Handheld style analog EPT
129.
Step Procedure
1 ️
1️⃣
Isolateand dry the tooth (avoid
saliva interference)
2️⃣
Apply conducting medium
(e.g., toothpaste) to probe tip
3 ️
3️⃣
Place probe on middle third
of facial surface
4️⃣
Instruct patient to signal when
sensation is felt
5 ️
5️⃣
Gradually increase current;
note the reading at first
response
Clinical Protocol
130.
FALSE RESPONSE
Patient relatedfactors
Tooth characteristics
Restored teeth
Supporting tissues
Apex maturation
Repeated trials
Psychological state
Physiological state
Failure to
complete the
circuit
Equipment
problems
Probe placement
Interface media
131.
Necrotic pulp respondsto
testing.
Stimulation of adjacent
teeth
The response of vital
tissue in multirooted tooth
with pulp necrosis in one
or more canals
Patient interpretation:
subjectivity
False positive & negative
Vital pulp that does not respond
to
stimulation
Inadequate contact with the
stimulus
Tooth calcification
Immature apical development
Traumatic injury
Subjective nature of the tests
Elderly patients – regressive
neural changes
Analgesics for pain
Traumatic injury
132.
LIMITATIONS
1. Subjective; measureonly nerve supply
2. Thermal tests: not effective in substantial secondary dentine
formation
3. Unreliability of tests: Immature apices, traumatic injuries, more
subjectivity in the young
4. No correlation with the histologic status
5. Difficult to administer & inconclusive in children
6. Weaker response- aged pulp
7. Extensive restorations, pulp recession, pulp calcification
8. Lack of reproducibility
133.
No informationon health
status/ integrity
Unreliable for immature teeth
Not suitable with full coverage
restorations
Chances of ventricular
fibrillation
134.
Response Clinical Meaning
Responseat low current Normal or reversible pulpitis
Delayed/high threshold
Possible degeneration or
calcification
No response at max output
Suggests pulp necrosis
(confirm with vitality test)
Interpretation of Responses
⚠️False positives may occur due to conduction
through periodontal tissues or restorations
⚠️False negatives in trauma, immature apex, or
calcified canals
135.
•Chief Complaint: Spontaneouspain in upper molar
•Cold Test: Lingering pain
•EPT: Positive
•Radiograph: Deep caries approaching pulp
•Diagnosis: Symptomatic irreversible pulpitis
•Treatment Plan: Root canal therapy
Reference: Clinical protocol adapted from Pathways of the Pulp, 12th ed.
Case Example
136.
Fiber Type StimulusPain Type
Clinical
Relevance
Aδ fibers Cold
Sharp,
localized
Reversible
pulpitis
C fibers Heat
Dull,
lingering
Irreversible
pulpitis
Neurophysiology of Pulp
137.
•Trauma cases: Neuralresponse may be absent despite
vital pulp
•Immature teeth: Incomplete innervation → false
negatives in EPT
•Use vitality tests (e.g., pulse oximetry) in such cases
Special Considerations
138.
Parameter Traditional EPT
AdvancedEPT
Techniques
Stimulus Delivery
Analog dial-
controlled current
with manual ramp-
up
Digitally calibrated
current with auto-
ramp and visual
feedback
Application
Medium
Toothpaste as
conductive medium
Electroconductive
gels, saline, or
direct-tooth metal
contact
Comparison of Traditional vs. Advanced
Electric Pulp Testing
139.
Electrode Contact
Buccal enamel
surface
Bridgedvia
endodontic files,
orthodontic
brackets, or metallic
restorations
Indication Scope
Vitality assessment
in intact teeth
Applicable in
crowned teeth,
calcified canals,
immature teeth, and
limited-access
situations
Parameter Traditional EPT
Advanced EPT
Techniques
140.
Interpretation
Patient reports
tingling ormild pain
at contact threshold
Some systems
record response
latency and voltage
thresholds digitally;
AI-assisted analysis
in research
Feedback Type Subjective only
Visual/auditory
signal + potential
digital response
logging
Parameter Traditional EPT
Advanced EPT
Techniques
141.
Portability
Typically corded or
bulky
Compact,wireless,
and battery-
operated handheld
units
Hybrid Use
Standalone
neurostimulation
Integrated with
LDF, pulse
oximetry, or
thermal tests for
multimodal pulp
evaluation
Limitations
Inaccurate in
traumatized or
immature teeth;
crown insulators
affect accuracy
Enhanced
adaptability but may
require training and
are not widely
available in all
practices
Parameter Traditional EPT
Advanced EPT
Techniques
143.
🔬 Histological Correlation
AdvancedInsights in Pulp
Vitality Testing
•Ricucci & Siqueira, Clin Oral Investig, 2014
Neural tests may fail in early pulpitis or trauma
•Key Insight: Vascular changes precede neural
degeneration during pulp inflammation.
•Clinical Implication: A non-responsive pulp may still
have vital vasculature.
144.
“The vitality ofthe pulp determines the
vitality of the tooth—choose your tests
wisely.”
LASER DOPPLER FLOWMETRY
1.Principle
• LDF is a non-invasive method that detects pulpal blood
flow using low-power laser light.
• When the laser beam enters the tooth, it scatters upon
hitting moving red blood cells in the pulp, causing a
Doppler shift in the frequency of reflected light.
• The reflected signal is processed to estimate blood flow.
Reference
Jafarzadeh H, Abbott PV. Review of pulp sensibility and vitality tests. Int Endod J. 2010;43(8):679–92.
147.
Components
• Laser source(typically helium-
neon or diode laser)
• Optical fibers to deliver and
collect light
• Photodetector and signal
processor
• Display monitor
148.
Clinical Significance
• Directlyassesses pulp vitality—unlike EPT or cold test,
which rely on neural response.
• Highly valuable in young permanent teeth, trauma cases, or
when other tests are inconclusive.
149.
Limitations
• Sensitive totooth movement and ambient light
interference
• Expensive and not widely available in clinical settings
• Difficult interpretation due to baseline flow variability
NoblettWC, et al. Evaluation of pulse oximetry and laser Doppler flowmetry as pulp vitality tests. J Endod. 1996;22(6):354–9.
150.
Advantages:
Painless diagnosisas compared to thermal & electric pulp
tests
Diagnosis of immature or traumatized teeth
Curve Interpretation
Clinical
Implication
Left Curve
Fluctuating
signal
indicating
active blood
flow
Vital pulp:
Normal
microcirculatio
n present
Right Curve
Flat signal
indicating
absence of
blood flow
Nonvital pulp:
No detectable
circulation
PULSE OXIMETRY
Principle
•Pulse oximetrymeasures the percentage of oxygenated
hemoglobin (SpO )
₂ in pulpal blood.
•A specialized sensor emits red and infrared light into the tooth;
the light absorbed reflects oxygen saturation levels, indicating
pulpal vitality.
Reference
Jafarzadeh H, Abbott PV. Review of pulp sensibility and vitality tests. Int Endod J. 2010;43(8):679–92.
153.
Components
•Modified pulse oximeterwith dental sensor
•LED light source (red and IR wavelengths)
•Photodetector for light absorption
•Digital display of SpO readings
₂
154.
• Probe containingtwo LEDs: red light- 660 nm
& infrared light (900–940 nm)
• Measures absorption of oxygenated and
deoxygenated Hb
• Received by a photodetector diode connected to a
microprocessor
• Relationship between the pulsatile change in the
absorption of red light & infrared light : assessed
by the oximeter
• known absorption curves for oxygenated and
deoxygenated hemoglobin
155.
•Provides direct assessmentof vascular integrity—
unlike cold or electric tests that rely on nerve response.
•Particularly valuable in:
•Immature teeth
•Recently traumatized teeth
•Pediatric patients
Clinical Relevance
156.
Inverse correlationbetween saturation values & EPT readings (Radhakrishnan et al 2002)
More sensitive & specific compared to cold tests & EPT (Gopikrishna et al 2007)
Indications:
Recent trauma
Primary &
immature
permanent teeth
157.
Limitations
•Requires customized intraoralsensors (commercial
options still evolving)
•Readings may vary due to tooth thickness, restorations,
or ambient light
•Interpretation needs a reference range (typically ~75–
85% for vital pulp)
Reference
Jafarzadeh H, Abbott PV. Review of pulp sensibility and vitality tests. Int Endod J. 2010;43(8):679–92.
158.
Inverse correlationbetween saturation values & EPT readings (Radhakrishnan et al 2002)
More sensitive & specific compared to cold tests & EPT (Gopikrishna et al 2007)
Limitations:
Intrinsic interference:
venous blood &
tissue constituents,
acidity,CO2
Extrinsic interference
Hb bound to other
gases
Extensive restorations
70%- 100% accuracy
159.
Device/System
Estimated Price
(INR)
Clinical UseReference
OxyTip+® with
Datex-Ohmeda
Monitor
₹1,50,000 –
3,00,000
₹
Used in studies
with custom
dental probe
holders
WJOUD Study –
Siddheswaran et
al.
GE B20 Pulse
Oximeter +
Dental Adapter
₹1,20,000 –
2,50,000
₹
Used in anterior
teeth vitality
studies
JCDR Study – Ba
ndaru et al.
Nellcor N-600x
with Custom
Probe
₹2,00,000 –
4,00,000
₹
Adapted for
pediatric and
traumatized teeth
JOCPD – Munshi
et al.
Masimo Radius
PPG Chip
(Research Use)
₹15,000 –
25,000
₹
Adaptable for
intraoral PPG-
based pulse
oximetry
IndiaMART
– Masimo Radiu
s
🦷 Pulse Oximetry Devices for Pulp
Vitality – India (2025)
160.
Comparative Summary ofPulp Testing
Methods
Patro S et al., 2022 – Systematic Review &
Meta-analysis
•Objective: Compared diagnostic accuracy of sensibility (cold,
EPT) vs. vitality tests (pulse oximetry, LDF)
•Findings:
• Pulse oximetry showed the highest sensitivity and
specificity
• Cold test was reliable but prone to false results in trauma
or immature teeth
• EPT had moderate accuracy and was less reliable in
young or calcified teeth
•Conclusion: Vitality tests are more accurate and objective
Patro S, Meto A, Mohanty A, Chopra V, Miglani S, Das A, Luke AM, Hadi DA, Meto A, Fiorillo L, Karobari MI.
Diagnostic accuracy of pulp vitality tests and pulp sensibility tests for assessing pulpal health in permanent
teeth: a systematic review and meta-analysis. International Journal of Environmental Research and Public
Health. 2022 Aug 4;19(15):9599.
161.
Dindaroğlu FC &Güngör NO, 2024 – Clinical Trial
•Objective: Compared cold test, EPT, and pulse oximetry in
mature vs. immature teeth
•Findings:
• Pulse oximetry was the only test that consistently
detected vitality in immature teeth
• Cold test and EPT gave false negatives in teeth with
open apices
•Conclusion: Pulse oximetry is superior in pediatric and
trauma cases
Çağırır Dindaroğlu F, Özay Güngör N. Comparison of the vitality test with sensitivity tests in mature and immature
teeth: clinical trial. BMC Oral Health. 2024 May 27;24(1):613.
162.
Tomer AK etal., 2019 – Narrative Review
•Objective: Reviewed traditional and modern pulp testing
methods
•Highlights:
• Emphasized the limitations of sensibility tests
• Advocated for pulse oximetry and LDF as future
standards
•Conclusion: Combining tests improves diagnostic accuracy
Tomer AK, Raina AA, Ayub F, Bhatt M. Recent advances in pulp vitality testing: A review. Int. J. Appl. Dent. Sci.
2019;5:8-12.
163.
Study & Year
Testing
Method
Clinical
Focus
Key
Conclusion
Ricucciet al.,
2014
Histology vs.
Clinical
Diagnosis
Vital and
inflamed pulp
correlation
Sensibility
test matched
histology in
84–96% of
cases
Radhakrishna
n et al., 2002
Pulse
Oximetry vs.
EPT
Pediatric pulp
vitality
PO produced
reproducible
readings
across age
groups
Comparative Evidence: Vascular vs.
Traditional Pulp Vitality Tests
164.
Evans et al.,
1999
LDFvs.
Traditional
Tests
Traumatized
anterior teeth
LDF showed
100%
sensitivity
and
specificity
Schnettler &
Wallace, 1991
Pulse
Oximetry
Vital vs.
endodontically
treated teeth
PO detected
oxygen
saturation
only in vital
pulps
Jafarzadeh,
2009
LDF (Review)
Literature
synthesis on
blood flow
testing
LDF is
objective,
non-invasive,
and highly
accurate
165.
Vongsavan &
Matthews,
1993
LDF on
Extracted
Teeth
Experimental
bloodflow
testing
LDF worked
well on
extracted teeth
with controlled
RBCs;
validates
flowmetry
conceptually.
Dastmalchi et
al., 2012
PO vs. Cold,
EPT, Rubber
Cup
Comparative
diagnostic
efficacy
Custom PO
probe delivered
91%
diagnostic
agreement;
superior across
patient cohorts.
166.
Rechenberg &
Zehnder, 2014
Molecular
Diagnostics
Futurepulp
vitality
strategies
Advocates
biomarker-
based testing
to surpass
neural response
limitations;
aligns with
next-gen
diagnostic
goals.
Rechenberg D-K, Zehnder M. Molecular diagnostics in endodontics. Endod Topics.
2014;30(1):51–65.
167.
DUAL WAVELENGTH
SPECTROPHOTOMETRY
Principle
•DWS measuresthe oxygen saturation of hemoglobin in
pulpal blood using two specific light wavelengths—typically
660 nm (red) and 940 nm (infrared).
•Oxygenated and deoxygenated hemoglobin absorb light
differently at these wavelengths. The device analyzes this
absorption to determine SpO levels, indicating pulpal
₂
vitality.
Reference
Jafarzadeh H, Abbott PV. Review of pulp sensibility and vitality tests. Int Endod J. 2010;43(8):679–92.
168.
Why Two Wavelengths?
•Thedual wavelength setup improves accuracy by
compensating for variables like tooth thickness,
translucency, and light scattering.
•It minimizes false readings that might occur with single-
wavelength devices.
169.
Clinical Benefits
•Non-invasive, objective,and suitable even when traditional
tests like cold/EPT are inconclusive.
•Useful in:
•Children with developing teeth
•Recently traumatized teeth
•Differentiating between necrosis and reversible pulpitis
170.
Limitations
•Still under clinicalevaluation and not widely available in
dental practice
•Sensor calibration and intraoral positioning require precision
•Influenced by light leakage or tooth discoloration
Jafarzadeh H,Abbott PV. Review of pulp sensibility and vitality tests. Int Endod J. 2010;43(8):679–92.
171.
System Type
Estimated Price
(INR)
ApplicationReference
Portable Dual-
Wavelength
Spectrophotome
ter
₹3,00,000 –
7,00,000
₹
General
biomedical use;
adaptable for
pulp testing
NewAge
Instruments
Benchtop UV-
VIS-NIR
Spectrophotome
ter
₹5,00,000 –
15,00,000
₹
Advanced lab
diagnostics,
including dental
research
IndiaMART – U
V-VIS Systems
Custom Dental
DWS Prototype
(Research Use)
Research-only
In vitro pulp
vitality studies
(e.g., Nissan et
al.)
Europe PMC – N
issan et al.
🧪 Dual Wavelength Spectrophotometry –
Estimated Price Range (India, 2025)
Nissan R, Trope M, Zhang CD, Chance B. Dual wavelength spectrophotometry as a diagnostic test of the pulp
chamber contents. Oral Surg Oral Med Oral Pathol. 1992;74(4):508–514.
172.
ULTRAVIOLET
LIGHT/FIBEROPTIC
FLUORESCENT SPECTROMETRY
Principle
•UV-FFS isbased on the natural fluorescence emitted by
biological tissues when stimulated by ultraviolet or blue light
(typically 400–500 nm).
•Vital pulp emits a different autofluorescence profile than
necrotic pulp due to the presence or absence of specific
metabolic byproducts.
173.
Technology Used
•A fiberopticprobe delivers UV or near-UV light into the
tooth structure.
•Emitted fluorescence is collected and measured by a
spectrometer to determine tissue vitality.
•Portable spectrometers and intraoral probes are being
developed for clinical use.
174.
Clinical Significance
•Non-invasive andreal-time method for assessing pulp
vitality.
•Especially useful in:
•Differentiating necrotic vs. inflamed pulp
•Early caries detection (as a bonus diagnostic application)
175.
Limitations
•Still in earlyexperimental stages for pulpal vitality
applications
•Results can be affected by tooth translucency, stains, and
restorations
•Requires specialized equipment not yet widely adopted
Sarma PK et al. Spectroscopic techniques in dental diagnostics. J Oral Sci. 2015;57(1):73–80.
PHOTOPLETHYSMOGRAPHY
Principle
•PPG is anon-invasive optical technique that measures
volume changes in blood microcirculation by detecting
variations in light absorption.
•Light-emitting diodes (LEDs) emit red or infrared light into
the tooth; the reflected light intensity fluctuates with each
pulse wave, indicating vascular activity in the pulp.
178.
How It Works
•Asensor containing an LED and photodetector is placed
on the tooth.
•Blood flow-related changes cause light absorption
variations, which are converted into electrical signals.
•These signals produce a waveform reflecting pulse
amplitude and rate.
179.
Clinical Utility
•Objective assessmentof pulp vitality based on real-time
vascular pulse
•Effective even when nerve response is unreliable—e.g., in
young permanent teeth, trauma cases, or elderly patients
•Portable and pain-free technique with potential for routine
use
180.
•Affected by motionartifacts and ambient light
•Requires calibration and adaptation for intraoral application
•Clinical validation in dentistry still ongoing
Chung SH, et al. Use of photoplethysmography to assess pulp vitality. J Endod.
2021;47(8):1225–30.
Limitations
181.
Instrument/
System
Estimated Price
(INR)
Application in
Dentistry
Reference
PPGI-basedPulp
Vitality System
Prototype /
Research-only
Intraoral imaging of
pulpal perfusion
Google Patents – U
S20210022593A1
Transmitted-Light
PPG (TLP) Setup
₹10,000 – 50,000
₹
(custom build)
Experimental use in
young permanent
teeth
AAPD Study – Mi
wa et al.
Masimo Radius
PPG Reusable
Chip
₹15,000 – 25,000
₹
Pulse rate and SpO₂
monitoring;
adaptable for
research
IndiaMART – Masi
mo Radius
Hokanson EC6
PPG System
₹1,90,000+
(approx. $2,300)
Research-grade
pulse waveform
analysis
Active Medical Sto
re
Wearable PPG
Devices (e.g.,
Shimmer, STARR)
₹1,00,000 –
3,00,000
₹
Biosignal
acquisition for
intraoral/fingertip
use
MedicalExpo
– PPG Devices
Photoplethysmography Instruments for
Dental Vitality Testing – India (2025)
182.
Feature
Laser
Doppler
Flowmetry
(LDF)
Pulse
Oximetry
(PO)
Photoplethys
mography
(PPG)
Principle
Measures red
blood cell
movementvia
Doppler shift
of laser light
Detects blood
oxygen
saturation via
absorption of
red/infrared
light
Detects blood
volume
changes via
reflected/trans
mitted light
Invasiveness Non-invasive Non-invasive Non-invasive
Sensor
Placement
Buccal/labial
surface near
tooth root
Tooth surface
+ reference on
soft tissue
Tooth surface,
crown, or
intraoral
adaptation
Comparative Overview of Vitality Testing
Technologies
TOOTH SURFACE TEMPERATURE
Principle
•Thismethod is based on the observation that vital teeth
maintain a slightly higher surface temperature than non-vital
teeth due to active pulpal blood flow.
•Temperature is measured using thermocouples,
thermistors, or infrared thermography.
Reference
Jafarzadeh H, Abbott PV. Review of pulp sensibility and vitality tests. Int Endod J. 2010;43(8):679–92.
186.
How It Works
•Atemperature sensor is placed on the buccal or labial surface
of the tooth.
•The reading is compared to adjacent or contralateral teeth.
•A lower temperature may indicate pulpal necrosis or
compromised blood flow.
187.
Clinical Applications
•Useful intrauma cases or when conventional tests are
inconclusive.
•Can be combined with other vitality tests for improved
diagnostic accuracy.
188.
Limitations
•Influenced by ambienttemperature, saliva, and enamel
thickness
•Requires controlled environmental conditions for reliable
results
•Not widely used in routine practice due to equipment
sensitivity
Udoye C. The Application of Tooth Temperature Measurement in Endodontic
Diagnosis: A Review. J Endod. 2008;34(9):1049–1052.
189.
Principle
•A thermistor isa temperature-sensitive resistor whose
electrical resistance changes with temperature.
•When placed in contact with the tooth, it detects subtle
thermal responses—vital teeth generate different temperature
patterns compared to necrotic ones.
Thermistor-Based Testing in
Pulp Vitality Assessment
190.
Mechanism of Action
•Thethermistor is applied to the tooth surface.
•It records temperature changes over time in
response to controlled thermal stimuli.
•The response curve helps differentiate between
vital and non-vital pulp.
191.
Clinical Significance
•Helps detectabnormal thermal conductivity in teeth
with questionable vitality.
•Non-invasive and painless.
•May enhance interpretation of cold/heat tests,
especially in research or complex cases.
Kimura Y, Wilder-Smith P. Thermographic analysis of pulpal response to thermal stimuli. J Dent Res.
2000;79(4):870–874
192.
• Affected byexternal temperature, saliva, and enamel
thickness
• Less commonly used due to availability of simpler tests (like
EPT or cold test)
• Needs calibration and specific probes for intraoral use.
Kimura Y, Wilder-Smith P. Thermographic analysis of pulpal response to thermal stimuli. J Dent Res.
2000;79(4):870–874
Limitations
193.
Principle
•Electronic thermography usesinfrared sensors to detect and
visualize temperature variations on the tooth surface.
•Vital teeth exhibit higher surface temperatures due to active
blood flow, while non-vital teeth show cooler profiles.
Electronic Thermography
194.
How It Works
•Aninfrared thermographic camera captures thermal
images of the tooth.
•These images are analyzed to detect asymmetries or
temperature drops that may indicate pulpal necrosis.
•Often used in comparative mode—comparing suspect teeth
with adjacent or contralateral teeth.
195.
Clinical Applications
•Non-invasive andcontact-free method
•Useful in:
•Diagnosing trauma cases
•Monitoring healing after revascularization
•Pediatric and geriatric patients where traditional tests may be
unreliable.
Dimitriu B, et al. Dental Pulp Assessment – The First Step Towards an Accurate Diagnostic in Endodontics.
Acta Scientific Medical Sciences. 2024;8(3):171–175.
196.
• Influenced byambient temperature, saliva, and enamel
thickness
• Requires controlled conditions and specialized
equipment
• Interpretation may vary based on operator experience
Dimitriu B, et al. Dental Pulp Assessment – The First Step Towards an Accurate Diagnostic in Endodontics.
Acta Scientific Medical Sciences. 2024;8(3):171–175.
Limitations
197.
• The HughesProbeye 4300 Thermal Video System is a
pioneering infrared imaging device developed by Hughes
Aircraft Company in the late 1960s and early 1970s.
• It was one of the earliest portable thermal imaging systems
designed for medical, industrial, and defense applications.
198.
•Tripod-mounted infrared scanner:Captures thermal
radiation emitted from surfaces.
•TV monitor output: Displays real-time thermal images.
•High sensitivity: Capable of detecting temperature
differences as small as 0.1°C.
•Medical utility: Used in early thermographic diagnostics to
detect vascular or nerve dysfunction by visualizing
asymmetrical temperature patterns on the skin.
199.
Relevance to Dentistry
Whilenot originally designed for dental use, the
Probeye 4300 laid the groundwork for modern
dental thermography, including:
•Non-invasive pulp vitality assessment
•Monitoring healing in traumatized teeth
•Identifying inflammation through thermal
asymmetry
200.
Historical Significance
The Probeye4300 represents a milestone in thermal imaging
technology. Its legacy continues in today’s infrared
thermographic cameras used in both medicine and dentistry
for non-contact diagnostics.
201.
Condition
Estimated
Price (USD)
Platform Notes
Used
(working)
$199.99eBay
Tested for
power; no
further
diagnostics 1
Used (as-is) $125.00 Machinio
Sold without
power-on
confirmation
2
💰 Estimated Price for Hughes Probeye 4300 (Used Units)
1.eBay. Hughes Model 4300 Probeye InfraredViewer [Internet]. eBay.com; 2025 [cited 2025 Jul 1].
2.Machinio. Used Hughes 4300 Probeye InfraredViewer Listings [Internet]. Machinio.com; 2025 [cited 2025 Jul 1].
202.
ULTRASOUND
Principle
• Ultrasound useshigh-frequency sound waves to evaluate
pulpal blood flow and tissue density.
• The reflected sound waves (echoes) vary depending on the
vitality and vascularity of the pulp tissue.
203.
How It Works
•A miniature ultrasound transducer is placed on the tooth
surface.
• Sound waves penetrate the tooth and reflect off internal
structures.
• The returning echoes are analyzed to detect vascular
pulsations or tissue changes.
204.
Clinical Applications
• Non-invasiveand radiation-free
• Useful in: Assessing traumatized or immature teeth
• Differentiating between vital and necrotic pulp
• Monitoring healing after regenerative procedures
Jafarzadeh H, Abbott PV. Review of pulp sensibility and vitality tests. Int
Endod J. 2010;43(8):679–92.
205.
Limitations
•Limited penetration incalcified or restored teeth
•Requires specialized intraoral probes
•Interpretation may vary based on operator experience
Jafarzadeh H, Abbott PV. Review of pulp sensibility and vitality tests. Int
Endod J. 2010;43(8):679–92.
206.
Ultrasound Machines forPulp
Vitality Assessment – India (2025)
Manufacturer /
Supplier
Device / Model Key Features
Estimated Price
(INR)
Potential Dental
Application
Mindray India Pvt.
Ltd.
Z60 Vet / Z50
• High-frequency
linear probe (7.5–
12 MHz)
• Color Doppler
• Portable, compact
unit
₹4,50,000 –
6,00,000
₹
• Pulp chamber
perfusion
• Periapical
vascularity
• Trauma
monitoring
GE Healthcare
India
Versana Active /
Logiq V2
• B-mode &
Doppler
• Pediatric presets
• Needle
visualization
₹5,00,000 –
7,50,000
₹
• Immature apex
visualization
• Regenerative
endodontics
• Chairside
diagnostics
Philips India Ltd.
Lumify Handheld
Ultrasound
• Android/iOS
compatible
• High-res imaging
• Cloud-based data
export
₹3,80,000 –
5,00,000
₹
• Emergency
trauma screening
• Pulp vitality in
pediatric cases
Fujifilm Sonosite
India
Edge II / iViz
• Point-of-care
ultrasound
(POCUS)
• Doppler-enabled
• Rugged, portable
design
₹6,50,000 –
9,00,000
₹
• Pediatric pulp
perfusion
• Dental trauma
triage
• Research-based
diagnostics
207.
ULTRASONIC DOPPLER
IMAGING
Principle
• UDIuses high-frequency ultrasound waves to detect blood
flow within the dental pulp.
• When ultrasound waves encounter moving red blood cells,
they reflect back with a Doppler frequency shift—this shift
is analyzed to assess vascular activity, indicating pulp
vitality.
208.
How It Works
•A miniature Doppler ultrasound probe is placed on the
tooth surface.
• The probe emits sound waves and captures the reflected
signals.
• The Doppler shift is converted into a visual or audible
signal representing pulpal blood flow.
209.
Clinical Applications
• Objective,non-invasive method for assessing pulp vitality
Especially useful in:
• Traumatized teeth
•Immature permanent teeth
•Cases with inconclusive sensibility test results
Dimitriu B, et al. Dental Pulp Assessment – The First Step Towards an Accurate Diagnostic. Acta Scientific
Medical Sciences. 2024;8(3):171–175.
210.
Limitations
•Requires specialized intraoralprobes
•Signal interpretation can be affected by
tooth structure and probe angulation
•Still under clinical validation for
routine dental use
211.
Machine Type EstimatedPrice Range (INR) Reference
Handheld Vascular Doppler ₹4,000 – 45,000
₹ IndiaMART Doppler Listings
Fetal Doppler Monitors ₹9,000 – 1,25,000
₹ HospitalStore Fetal Doppler Guid
e
Portable Color Doppler
Ultrasound
₹3,00,000 – 9,00,000
₹ Bajaj Finserv Ultrasound Price Li
st
High-End Color Doppler
Systems
₹10,00,000 – 25,00,000+
₹ HospitalStore Full Price Guide
3D/4D Doppler Ultrasound
Machines
₹5,00,000 – 16,00,000
₹
ExportersIndia
Ultrasound Listings
Ultrasonic Doppler Imaging
Machine – Price Overview (India,
2025)
212.
OPTICAL REFLECTION
VITALOMETRY
Principle
•ORV isa non-invasive technique that detects pulsatile blood
flow in the dental pulp by analyzing light reflected from the
tooth surface.
•A light source (typically red or near-infrared) is directed at the
tooth, and the reflected light is measured to detect minute
changes in intensity caused by pulpal blood pulsations.
213.
How It Works
•Afiberoptic probe delivers light to the tooth and collects the
reflected signal.
•The signal is processed to identify rhythmic fluctuations
corresponding to the cardiac pulse, indicating vascular
vitality.
214.
Clinical Applications
•Objective assessmentof pulp vitality, especially in:
• Traumatized teeth
• Immature permanent teeth
• Cases with inconclusive sensibility test results
•Non-invasive and painless, with potential for chairside use.
215.
Limitations
•Affected by toothtranslucency, enamel thickness, and
ambient light
•Requires precise probe positioning and calibration
•Still under research and not yet widely available in clinical
practice
Herrala E. Detection of pulse in oral mucosa and dental pulp by means of optical reflection method. Dental
Traumatology. 1996.
216.
Patient Presents withSymptoms?
└── Yes → Clinical + Radiographic Evaluation
└── No → Routine Cold Test + Percussion
Cold Test Response?
├── Sharp, brief pain → Reversible Pulpitis
├── Lingering pain (>10s) → Symptomatic Irreversible
Pulpitis └── No response → EPT or Vitality Testing
Condition Preferred TestsNotes
Traumatized
teeth
Pulse oximetry,
LDF
Sensibility tests
often yield false
negatives
Immature apex
Pulse oximetry,
LDF
EPT is unreliable
due to incomplete
nerve
development
Calcified canals
Pulse oximetry,
LDF
Sensibility tests
may not detect
nerve signals
Special Scenarios
Accuracy of pulse oximetry and laser Doppler flowmetry in assessing pulp vitality – A comprehensive
review.” Int J Appl Dent Sci, 2021; 7(1): 11–15.
219.
Test Sensitivity SpecificityClinical Use
Cold Test High Moderate
First-line,
quick
screening
Electric Pulp
Test
Moderate Moderate
Useful in
mature teeth
Pulse
Oximetry
High High
Objective,
reliable in
trauma
Laser
Doppler
Flowmetry
Very High Very High
Research-
grade,
trauma/immat
ure teeth
Comparative Accuracy of Tests
Petersson et al., J Endod, 1999; Gopikrishna et al., 2009
220.
✅ Pulp vitality≠ neural response — true vitality is
defined by vascular integrity
✅ Traditional sensibility tests (thermal, EPT) are
subjective and prone to diagnostic pitfalls
✅ Advanced vitality tests (pulse oximetry, LDF) offer
objective, reliable insights into pulpal health
Summary & Clinical Takeaways
221.
✅ Diagnostic accuracyimproves when pulp testing is integrated
with radiographic findings, clinical signs, and patient history
✅ Special cases (trauma, immature apex, calcifications) require
tailored testing—vitality methods are preferred
222.
✅ A combinedtesting strategy ensures evidence-based,
minimally invasive, and predictable endodontic outcomes
✅ Emerging technologies (AI, photoacoustic imaging) may
soon redefine clinical diagnostics
223.
REFERENCES
• Weine FS.Endodontic therapy. 6th ed. St. Louis: Mosby;
2003.
• Ingle JI, Bakland LK, Baumgartner JC. Ingle's endodontics.
6th ed. Hamilton: BC Decker Inc; 2008.
• Cohen S, Hargreaves KM. Pathways of the pulp. 10th ed. St.
Louis: Mosby Elsevier; 2011.
• Grossman LI, Oliet S, Del Rio CE. Endodontic practice.
13th ed. Philadelphia: Wolters Kluwer; 2015.
• Pitt Ford TR. Endodontics: problem-solving in clinical
practice. London: Martin Dunitz; 2002.
224.
• Bessner C,Ferrigno S. Practical endodontics: a clinical guide.
New York: Thieme; 2005.
• Beer R. Pocket atlas of endodontics. Stuttgart: Thieme; 2006.
• Jafarzadeh H, Abbott PV. Review of pulp sensibility tests. Part
I: general information and thermal tests. Int Endod J.
2010;43(9):738–62.
• Yoon SY, Lee SJ, Kim E, Kang MK, Kim KD. Sensibility test
responses in vital and nonvital teeth: a clinical study. J Endod.
2010;36(3):375–8.
• Jespersen JJ, Hellstein JW, Johnson WT, Qian F. Evaluation of
dental pulp sensibility tests in a clinical setting. J Endod.
2014;40(3):351–5.
• Sharma S, Chopra R, Srivastava D, Bhatia A. Comparison of
pulse oximetry and laser Doppler flowmetry in assessing pulp
vitality. Int J Appl Dent Sci. 2021;7(1):11–15.
• Gopikrishna V, Tinagupta K, Kandaswamy D. Evaluation of
efficacy of a pulse oximeter in assessing pulp vitality. Int J
Paediatr Dent. 2007;17(2):56–61.
#13 Art: It involves clinical intuition, experience, and judgment. Science: It relies on objective data, tests, and evidence-based reasoning.
Deviations from health: Refers to any abnormal signs, symptoms, or test results.
Cause and nature: Involves identifying the underlying pathology or condition responsible.
#14 Afte reaching the pulpal diagnosis which may be due to
Therefore it is imp to perform the pulp vitality
#16 Pulp vitality tests (cold, heat, EPT) are only meaningful when interpreted alongside patient history. Helps differentiate pulpal pain from referred, periodontal, or non-dental origins.
Informs the selection and sequencing of diagnostic tests.
Name-accurate patient identification Prevents mix-ups
Address-geographic access to care, especially for follow-up in pulp vitality cases
#17 Localizes the problem and identifies triggering stimuli (e.g., cold, heat, biting)
#20 “needle-like” sensation
rhythmic, pulsing sensation
Lancinating pain is a sudden, sharp, stabbing sensation
Aching pain is typically described as a dull, persistent, and often diffuse discomfort.
Gnawing pain is often described as a deep, persistent, and nagging discomfort
#84 American Association of Endodontists. AAE Position Statement on Vital Pulp Therapy. Chicago: AAE; 2021.
🧒 American Academy of Pediatric Dentistry (AAPD)
Coll JA, Dhar V, Chen CY, et al. Use of Vital Pulp Therapies in Primary Teeth with Deep Caries: 2024 Clinical Practice Guideline. Pediatr Dent. 2024;46(1):13–26.
European Society of Endodontology. European Society of Endodontology position statement: Management of deep caries and the exposed pulp. Int Endod J. 2019;52(7):923–34.
Sachdeva A, Kumar V, Chawla A, et al. Quality assessment of clinical practice guidelines and position statements on vital pulp therapy: A systematic review. Evid Based Dent. 2025.
#85 American Association of Endodontists. AAE Position Statement on Vital Pulp Therapy. Chicago: AAE; 2021.
🧒 American Academy of Pediatric Dentistry (AAPD)
Coll JA, Dhar V, Chen CY, et al. Use of Vital Pulp Therapies in Primary Teeth with Deep Caries: 2024 Clinical Practice Guideline. Pediatr Dent. 2024;46(1):13–26.
European Society of Endodontology. European Society of Endodontology position statement: Management of deep caries and the exposed pulp. Int Endod J. 2019;52(7):923–34.
Sachdeva A, Kumar V, Chawla A, et al. Quality assessment of clinical practice guidelines and position statements on vital pulp therapy: A systematic review. Evid Based Dent. 2025.
#145 Red light is emitted from a light source; if the light beam is scattered-off of stationary tissue or cells, there is no shift in the light spectrum. If, however, the light hits a moving cell in a blood vessel there is a shift in the light spectrum of the scattered light according to the Doppler flowmetry
#153 Left Side – Sensor Mechanics
Light Sources (a & b):
Emit two specific wavelengths: red (~660 nm) and infrared (~940 nm).
These penetrate through the tissue (or enamel/dentin in dental adaptation).
Tissue Interaction:
Oxygenated hemoglobin absorbs infrared, while deoxygenated absorbs red.
The diagram shows layered tissue, representing vascular zones where light absorption occurs.
Photodetector (f):
Captures transmitted/reflected light after passing through the tissue.
Signals are processed to compute oxygen saturation (SpO₂).
📊 Right Side – Display Output
Graphical Peaks: Correspond to absorbance at the two wavelengths.
“560” is likely a stylized label but true measurements occur at 660 and 940 nm.
SpO₂ Value:
The display shows “82” as an oxygen saturation percentage.
In dental pulp testing, values below 90% may indicate reduced vitality. Display Unit (d):
Represents the pulse oximeter screen showing live readings.
#159 📚 Vancouver Style References
Radhakrishnan S, Munshi AK, Hegde AM. Pulse oximetry: a diagnostic instrument in pulpal vitality testing. J Clin Pediatr Dent. 2002;26(2):141–145.
Dastmalchi N, Jafarzadeh H, Moradi S. Comparison of the efficacy of a custom-made pulse oximeter probe with digital electric pulp tester, cold spray, and rubber cup for assessing pulp vitality. J Endod. 2012;38(9):1182–1186.
Sabharwal RJ, Dhull KS, Dutta B, et al. Evaluation of pulp vitality using pulse oximetry: a systematic review and meta-analysis. Int J Clin Pediatr Dent. 2025;18(4):479–486.
Siddheswaran V, Adyanthaya R, Shivanna V. Pulse oximetry: a diagnostic instrument in pulpal vitality testing—an in vivo study. World J Oral Dent. 2023;14(1):12–18.
Dutta SD, Maria R. Pulse oximetry: a new tool in pulpal vitality testing. Peoples J Sci Res. 2013;6(1):35–39.
Would you like a comparative schematic slide illustrating how PO integrates into the pulp testing workflow—or a reference sheet linking these devices with clinical studies? I’d be delighted to help craft those next 🦷📊✨
#163 Ricucci D, Loghin S, Siqueira JF Jr. Correlation between clinical and histologic pulp diagnoses. J Endod. 2014;40(12):1932–1939
Radhakrishnan S, Munshi AK, Hegde AM. Pulse oximetry: a diagnostic instrument in pulpal vitality testing. J Clin Pediatr Dent. 2002;26(2):141–145.
#164 Evans D, Reid J, Strang R, Stirrups D. A comparison of laser Doppler flowmetry with other methods of assessing vitality of traumatised anterior teeth. Endod Dent Traumatol. 1999;15(6):284–290
Schnettler JM, Wallace JA. Pulse oximetry as a diagnostic tool of pulpal vitality. J Endod. 1991;17(10):488–490.
Jafarzadeh H. Laser Doppler flowmetry in endodontics: a review. Int Endod J. 2009;42(6):476–490.
#165
Vongsavan N, Matthews B. Some aspects of the use of laser Doppler flow meters for recording tissue blood flow. Exp Physiol. 1993;78(1):1–14.
Dastmalchi N, Jafarzadeh H, Moradi S. Comparison of the efficacy of a custom-made pulse oximeter probe with digital electric pulp tester, cold spray, and rubber cup for assessing pulp vitality. J Endod. 2012;38(9):1182–1186.
#181 📚 Vancouver-Style References
Dory R, Bequette JP, Tewolde S. Photoplethysmography Imaging (PPGI)-Based Pulp Vitality Test. US Patent Application US20210022593A1. 2021 Jan 28.
Sabharwal RJ, Dhull KS, Dutta B, et al. Evaluation of pulp vitality using pulse oximetry: a systematic review and meta-analysis. Int J Clin Pediatr Dent. 2025;18(4):479–486.
Siddheswaran V, Adyanthaya R, Shivanna V. Pulse oximetry: a diagnostic instrument in pulpal vitality testing—an in vivo study. World J Oral Dent. 2023;14(1):12–18.
Core Market Research. India Dental Examination Devices Market Forecast 2025–2031 [Internet]. [cited 2025 Jul 7].
#182 Miwa et al., AAPD. Transmitted-light PPG in young permanent teeth. Pediatr Dent. 2002.
Dory et al., PPGI-based pulp testing. US Patent US20210022593A1.
Appel & Theart, Design of a PPG device. Sensors (Basel). 2025.
Ingle’s Endodontics (7th ed.), Chapter on Vitality Testing.
Cohen’s Pathways of the Pulp (12th ed.), Diagnostic Modalities secti
#183 Miwa et al., AAPD. Transmitted-light PPG in young permanent teeth. Pediatr Dent. 2002.
Dory et al., PPGI-based pulp testing. US Patent US20210022593A1.
Appel & Theart, Design of a PPG device. Sensors (Basel). 2025.
Ingle’s Endodontics (7th ed.), Chapter on Vitality Testing.
Cohen’s Pathways of the Pulp (12th ed.), Diagnostic Modalities secti
#184 Miwa et al., AAPD. Transmitted-light PPG in young permanent teeth. Pediatr Dent. 2002.
Dory et al., PPGI-based pulp testing. US Patent US20210022593A1.
Appel & Theart, Design of a PPG device. Sensors (Basel). 2025.
Ingle’s Endodontics (7th ed.), Chapter on Vitality Testing.
Cohen’s Pathways of the Pulp (12th ed.), Diagnostic Modalities secti
#206 Dutta SD, Maria R. Ultrasound in endodontics: a review of emerging diagnostic applications. J Conserv Dent. 2023;26(2):101–107.
Ricucci D, Loghin S, Siqueira JF Jr. Correlation between clinical and histologic pulp diagnoses. J Endod. 2014;40(12):1932–1939.
Rechenberg D-K, Zehnder M. Molecular diagnostics in endodontics. Endod Topics. 2014;30(1):51–65.
Core Market Research. India Ultrasound Devices Market Forecast 2025–2031 [Internet]. [cited 2025 Jul 7]. Available from: India Ultrasound Devices Market Size | Mordor Intelligence
Sabharwal RJ, Dhull KS, Dutta B, et al. Evaluation of pulp vitality using pulse oximetry: a systematic review and meta-analysis. Int J Clin Pediatr Dent. 2025;18(4):479–486.

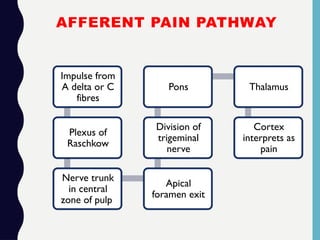
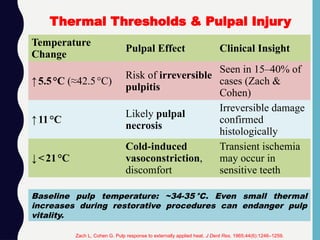
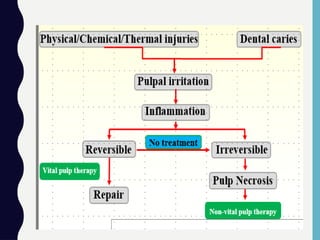
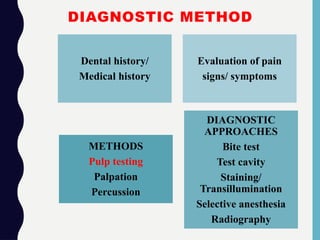
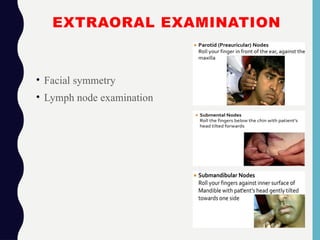
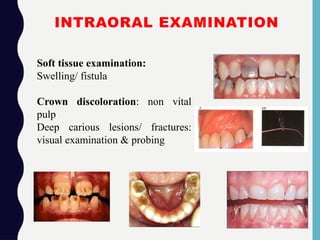
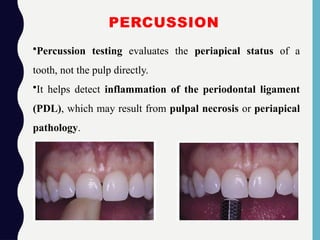
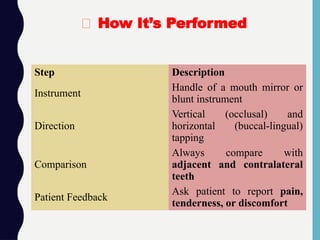
![Response Clinical Implication
No pain
Normal PDL and likely
healthy pulp
Mild discomfort
Possible early inflammation
or occlusal trauma
Sharp pain on percussion
Suggests periapical
inflammation, often due to
pulpal necrosis
Pain on lateral percussion
May indicate cracked tooth
syndrome or periodontal
involvement
🧠 Interpretation of Responses
1.Hargreaves KM, Berman LH. Cohen’s Pathways of the Pulp. 11th ed. St. Louis: Elsevier; 2016. p. 92–95.
2.Torabinejad M, Walton RE. Endodontics: Principles and Practice. 5th ed. Saunders; 2014. p. 108–110.
2.Animated Teeth. Root canal testing – percussion, thermal, and electric pulp tests [Internet]. 2023 [cited 2025 Jul 4].](https://image.slidesharecdn.com/pulpvitalitytestadvances-260203202935-01f00d35/85/Pulp-Vitality-Test-Advances-pptxaaaaaaaaaaaaaa-31-320.jpg)
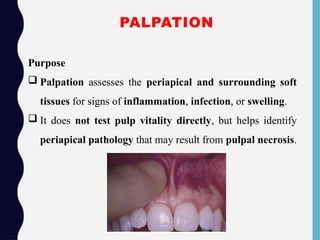
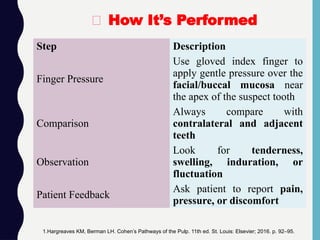
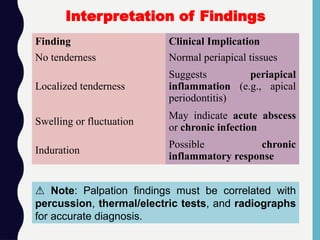

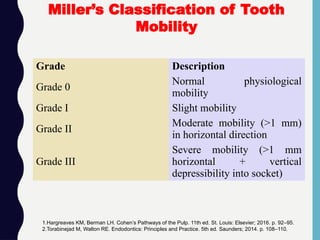
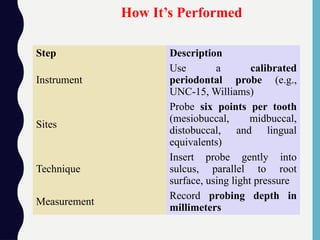
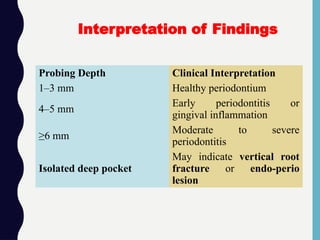
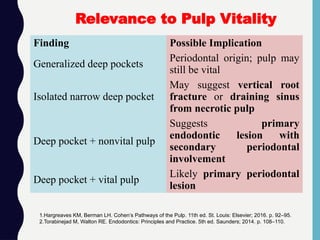
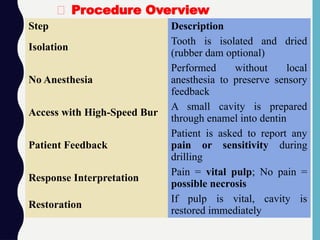
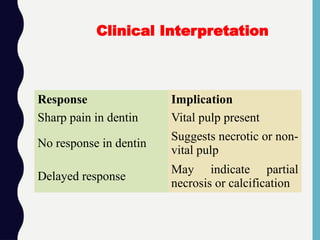
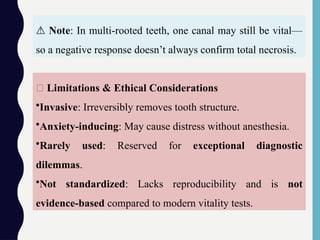
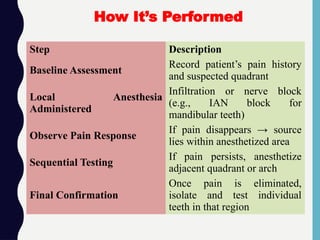
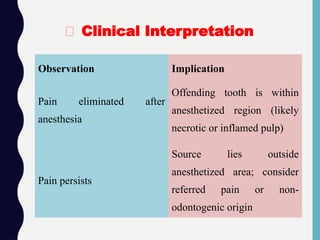
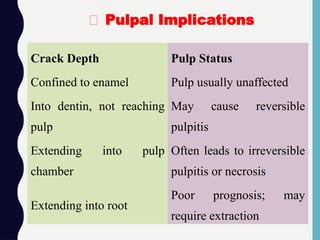
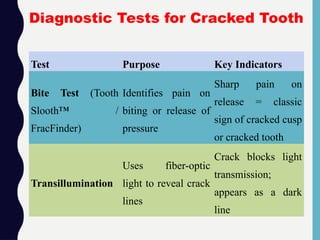
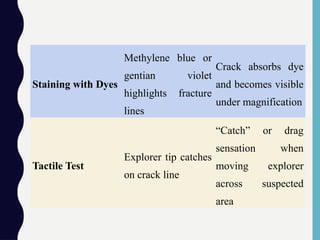
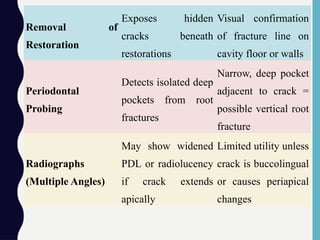
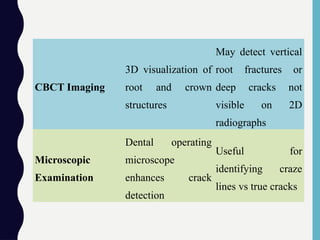
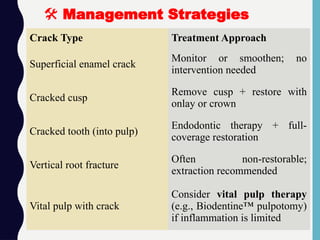
![•Pain on release (not just on biting) is a hallmark of cracked
tooth syndrome.
•Always test each cusp individually using a bite stick to
localize the crack.
•Combine tests for higher diagnostic accuracy—e.g.,
transillumination + staining + bite test.
1.Markose A. Crack tooth syndrome: Diagnosis and management [Internet]. IOSR J Dent Med Sci. 2020 [cited 2025
Jul 4];19(10):4–9.](https://image.slidesharecdn.com/pulpvitalitytestadvances-260203202935-01f00d35/85/Pulp-Vitality-Test-Advances-pptxaaaaaaaaaaaaaa-56-320.jpg)
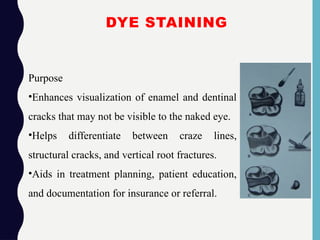
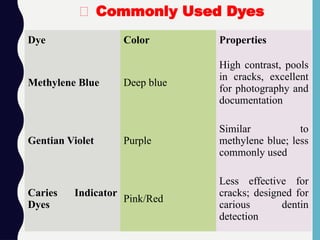
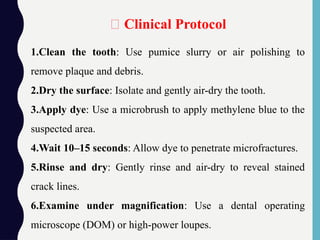
![🧠 Tip: Dye staining is especially useful after removing
restorations, as many cracks originate beneath amalgams or
composites.
1.Markose A. Crack tooth syndrome: Diagnosis and management [Internet]. IOSR J Dent Med Sci. 2020 [cited
2025 Jul 4];19(10):4–9.](https://image.slidesharecdn.com/pulpvitalitytestadvances-260203202935-01f00d35/85/Pulp-Vitality-Test-Advances-pptxaaaaaaaaaaaaaa-60-320.jpg)
![•May overstain plaque or sodium hypochlorite-treated dentin.
•Cannot differentiate between active vs. inactive cracks.
•May mask subtle color changes when used with
transillumination.
Limitations
1.Markose A. Crack tooth syndrome: Diagnosis and management [Internet]. IOSR J Dent Med Sci. 2020 [cited
2025 Jul 4];19(10):4–9.](https://image.slidesharecdn.com/pulpvitalitytestadvances-260203202935-01f00d35/85/Pulp-Vitality-Test-Advances-pptxaaaaaaaaaaaaaa-61-320.jpg)
![Why It Works
•Biting separates the crack, stimulating A-delta fibers in
dentin.
•Releasing pressure causes rebound movement, triggering
sharp pain.
1.Markose A. Crack tooth syndrome: Diagnosis and management [Internet]. IOSR J
Dent Med Sci. 2020 [cited 2025 Jul 4];19(10):4–9.](https://image.slidesharecdn.com/pulpvitalitytestadvances-260203202935-01f00d35/85/Pulp-Vitality-Test-Advances-pptxaaaaaaaaaaaaaa-65-320.jpg)
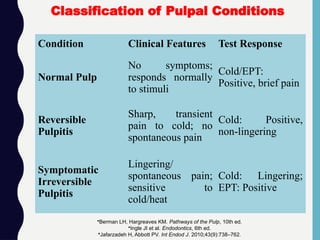
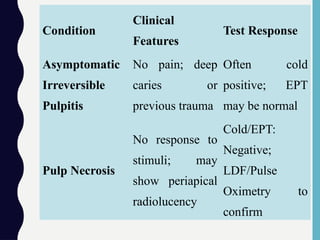
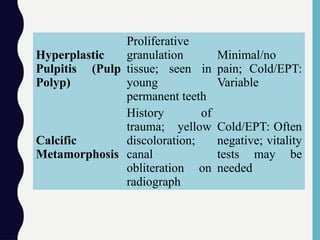
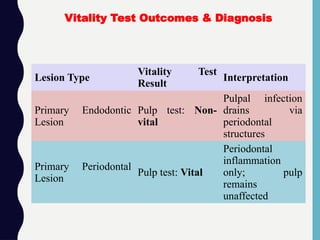
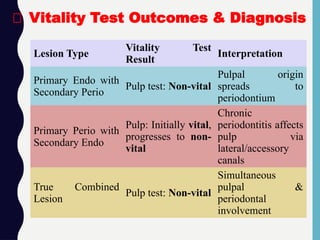
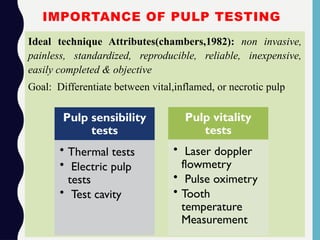
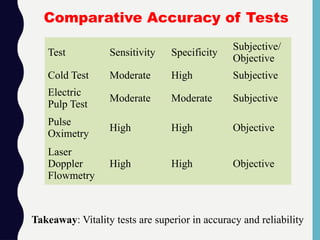
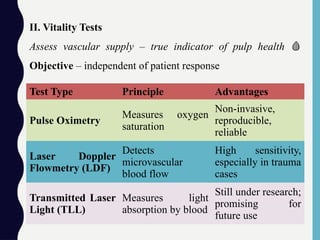
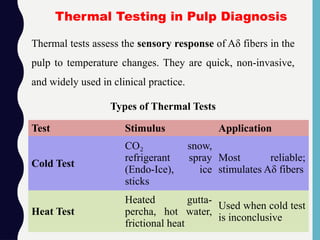
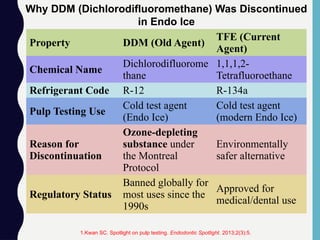
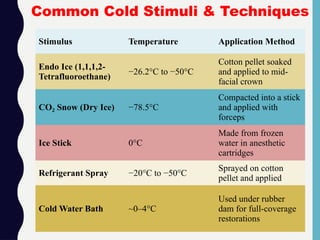
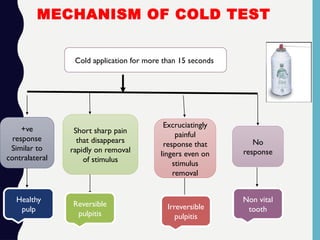
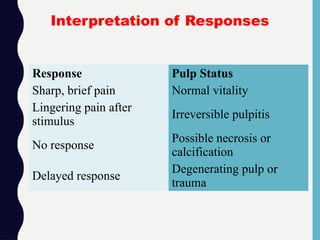
![•Sensitivity: ~89%
•Specificity: ~83%
•Most accurate among sensibility tests for detecting vital
pulp, especially in anterior teeth.
Diagnostic Accuracy
Decisions in Dentistry. Principles of endodontic diagnosis [Internet]. 2022 [cited 2025 Jul 4]](https://image.slidesharecdn.com/pulpvitalitytestadvances-260203202935-01f00d35/85/Pulp-Vitality-Test-Advances-pptxaaaaaaaaaaaaaa-111-320.jpg)
![•Subjective: Depends on patient perception.
•False negatives: Common in calcified, traumatized, or
immature teeth.
•False positives: May occur due to anxiety or adjacent
tooth conduction.
Decisions in Dentistry. Principles of endodontic diagnosis [Internet]. 2022 [cited 2025 Jul 4]
⚠️Limitations](https://image.slidesharecdn.com/pulpvitalitytestadvances-260203202935-01f00d35/85/Pulp-Vitality-Test-Advances-pptxaaaaaaaaaaaaaa-112-320.jpg)
![Parameter
Traditional
Methods
Advanced
Methods
Examples
Endo Ice, Dry Ice,
Ice Stick, Cold
Water Bath
Calset™ Digital
Cold Tester,
Modified
Tetrafluoroethane
Sprays
Temperature
Control
Unregulated;
manually chilled
materials (~−26°C
to 0°C)
Digitally calibrated
devices (~−50°C)
with precise
temperature and
timing control
Comparison of Traditional and Advanced Cold
Test Methods
1.Adam M. ‘Cold is gold’? The diagnostic accuracy of sensibility and vitality testing techniques [Internet]. Evid Based
Dent. 2022 [cited 2025 Jul 4];23:137.](https://image.slidesharecdn.com/pulpvitalitytestadvances-260203202935-01f00d35/85/Pulp-Vitality-Test-Advances-pptxaaaaaaaaaaaaaa-113-320.jpg)
![Parameter
Traditional
Methods
Advanced
Methods
Stimulus
Consistency
Operator-dependent
Standardized across
applications using
calibrated systems
Response
Monitoring
Patient's
verbal/subjective
report
Experimental AI-
assisted latency and
pain-intensity
analysis
Application
Feedback
None
Integrated thermal
imaging to track
application area and
temperature spread
1.Adam M. ‘Cold is gold’? The diagnostic accuracy of sensibility and vitality testing techniques [Internet]. Evid Based
Dent. 2022 [cited 2025 Jul 4];23:137.](https://image.slidesharecdn.com/pulpvitalitytestadvances-260203202935-01f00d35/85/Pulp-Vitality-Test-Advances-pptxaaaaaaaaaaaaaa-114-320.jpg)
![Clinical Challenges
Difficult in
heavily restored
or calcified teeth
Improved
performance in
cases of trauma,
open apex, or
multi-surface
restorations
Interpretation Bias
High; depends
solely on patient
feedback
Reduced with
integrated
multimodal
tools (e.g.,
combining with
Pulse Oximetry
or LDF)
1.Adam M. ‘Cold is gold’? The diagnostic accuracy of sensibility and vitality testing techniques [Internet]. Evid Based
Dent. 2022 [cited 2025 Jul 4];23:137.](https://image.slidesharecdn.com/pulpvitalitytestadvances-260203202935-01f00d35/85/Pulp-Vitality-Test-Advances-pptxaaaaaaaaaaaaaa-115-320.jpg)
![Availability
Widely
available, low
cost
Limited clinical
use (research
phase for
some), requires
investment in
newer tech
1.Adam M. ‘Cold is gold’? The diagnostic accuracy of sensibility and vitality testing techniques [Internet]. Evid Based
Dent. 2022 [cited 2025 Jul 4];23:137.](https://image.slidesharecdn.com/pulpvitalitytestadvances-260203202935-01f00d35/85/Pulp-Vitality-Test-Advances-pptxaaaaaaaaaaaaaa-116-320.jpg)
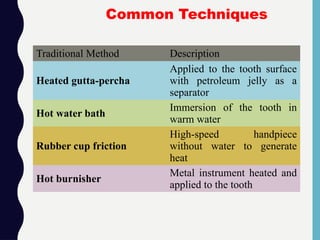
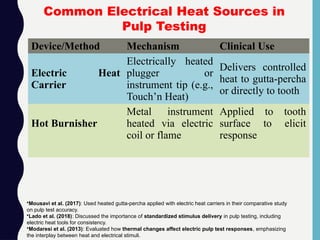
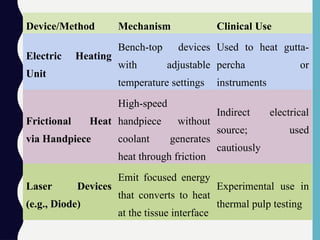
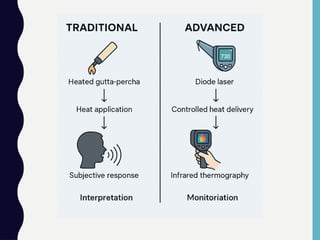
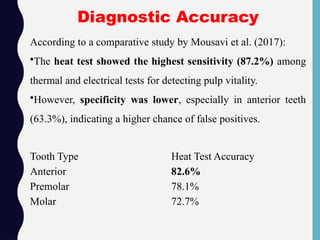
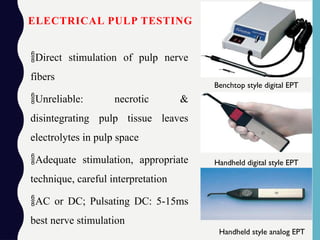
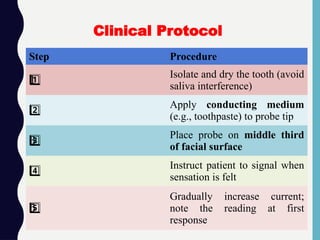

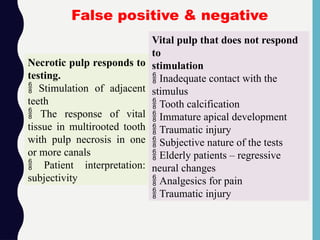
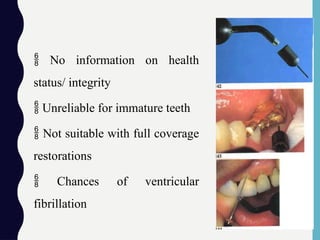
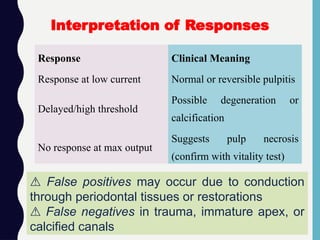
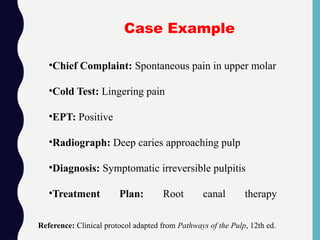
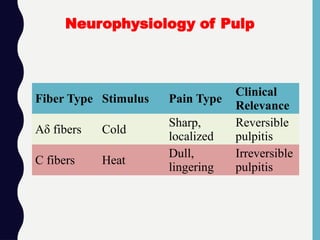
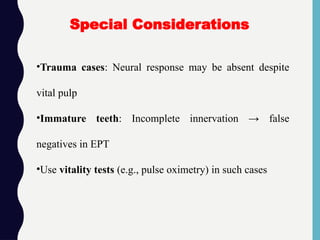
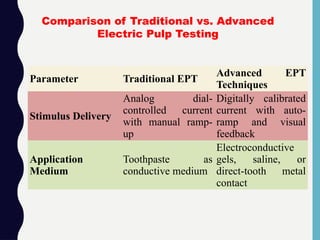
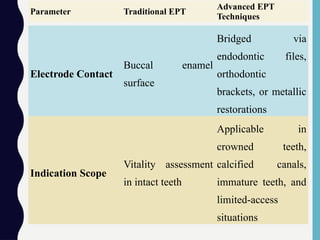
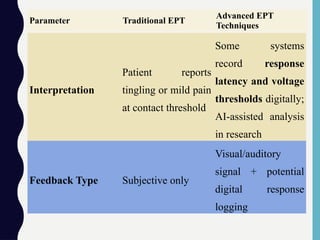
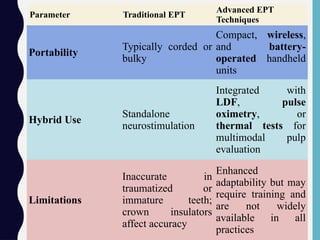
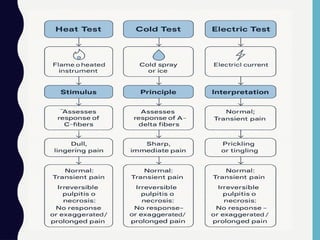
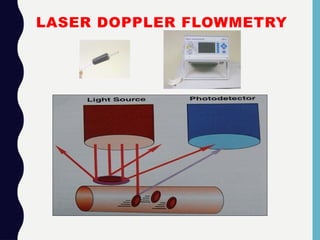
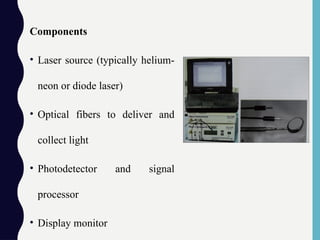
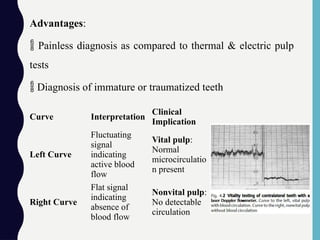
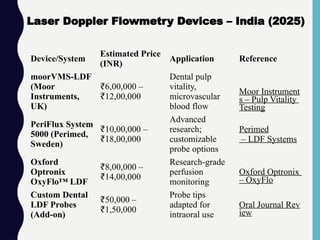
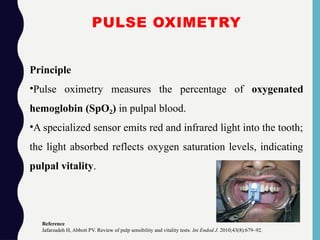
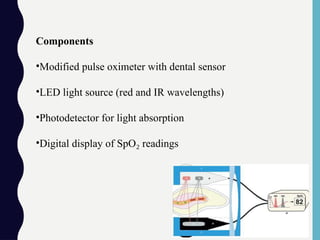
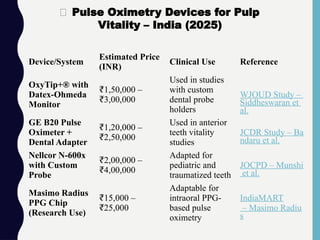
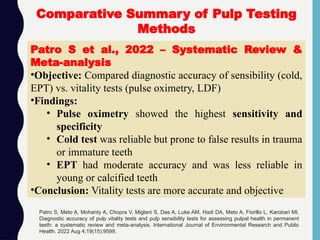
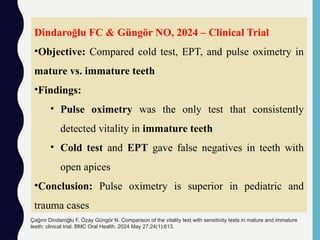
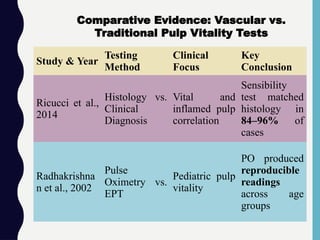
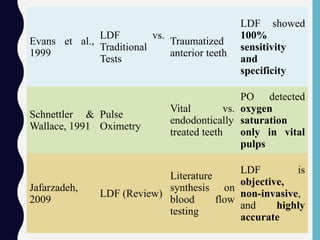
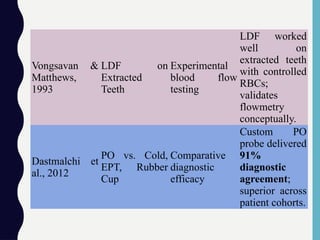
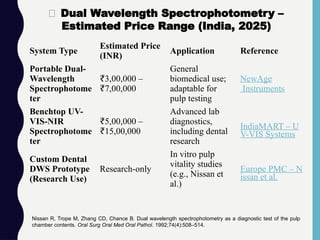
![System/Instrument
Estimated Price
(INR)
Application Reference
Fiber Optic
Spectrometer (UV-
VIS/NIR)
₹3,50,000 –
10,00,000
₹
Fluorescence,
reflection, and
absorbance analysis
NewAge Instruments
Mini Spectrometer
(SMD Series)
₹22,000 – 1,00,000
₹
Compact
fluorescence
detection (640–1050
nm)
NewAge Instruments
Transmission Dip
Probe (UV-VIS)
₹1,00,000+
Intraoral light
delivery and signal
collection
NewAge Instruments
Multi-Channel
Fluorescence
Spectrometer
₹10,00,000+
Advanced research;
multi-wavelength
fluorescence
NewAge Instruments
UV/Fiberoptic Fluorescent
Spectrometry in Pulp Vitality
Testing
Oral Journal. Recent advances in pulp vitality testing: A review [Internet]. 2019 [cited 2025 Jul 1].](https://image.slidesharecdn.com/pulpvitalitytestadvances-260203202935-01f00d35/85/Pulp-Vitality-Test-Advances-pptxaaaaaaaaaaaaaa-176-320.jpg)
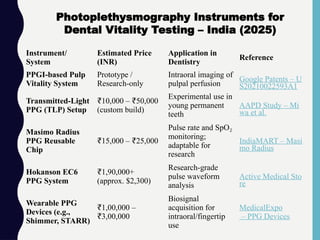
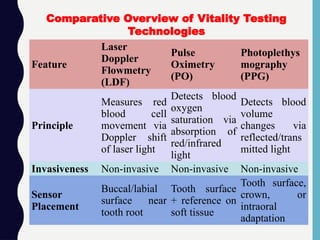
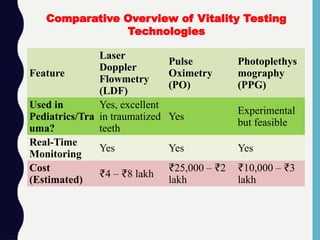
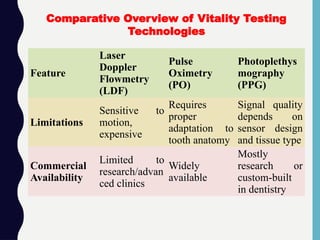
![Condition
Estimated
Price (USD)
Platform Notes
Used
(working)
$199.99 eBay
Tested for
power; no
further
diagnostics 1
Used (as-is) $125.00 Machinio
Sold without
power-on
confirmation
2
💰 Estimated Price for Hughes Probeye 4300 (Used Units)
1.eBay. Hughes Model 4300 Probeye InfraredViewer [Internet]. eBay.com; 2025 [cited 2025 Jul 1].
2.Machinio. Used Hughes 4300 Probeye InfraredViewer Listings [Internet]. Machinio.com; 2025 [cited 2025 Jul 1].](https://image.slidesharecdn.com/pulpvitalitytestadvances-260203202935-01f00d35/85/Pulp-Vitality-Test-Advances-pptxaaaaaaaaaaaaaa-201-320.jpg)
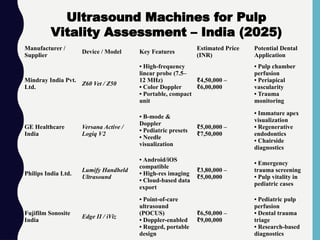
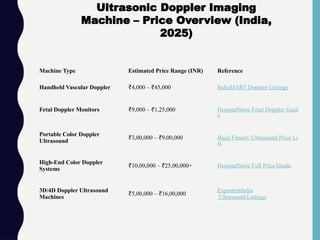
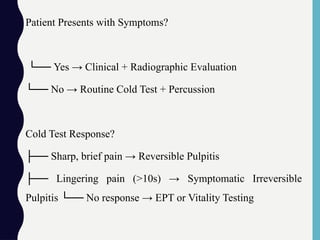
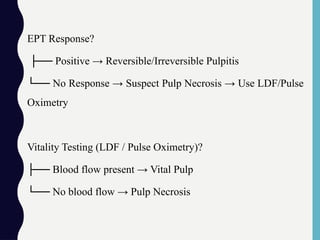
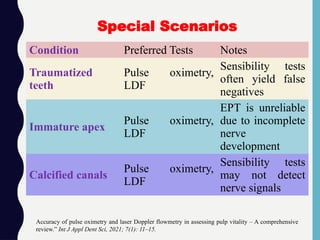
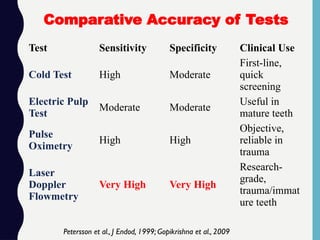












![endo diagnosis ppt friday.pptx [Autosaved].pptx](https://cdn.slidesharecdn.com/ss_thumbnails/endodiagnosispptfriday-240220084902-bcb16ad0-thumbnail.jpg?width=640&height=640&fit=bounds)






























![ONFH[AVN HIP] -TRIPLE REGIME -A NOVAL SURGICAL CONCEPT .pptx](https://cdn.slidesharecdn.com/ss_thumbnails/onfhavnhip2026koaconcalicutdrgokuldevdrmashraf-260210064517-213ec005-thumbnail.jpg?width=640&height=640&fit=bounds)



