Downloaded 733 times
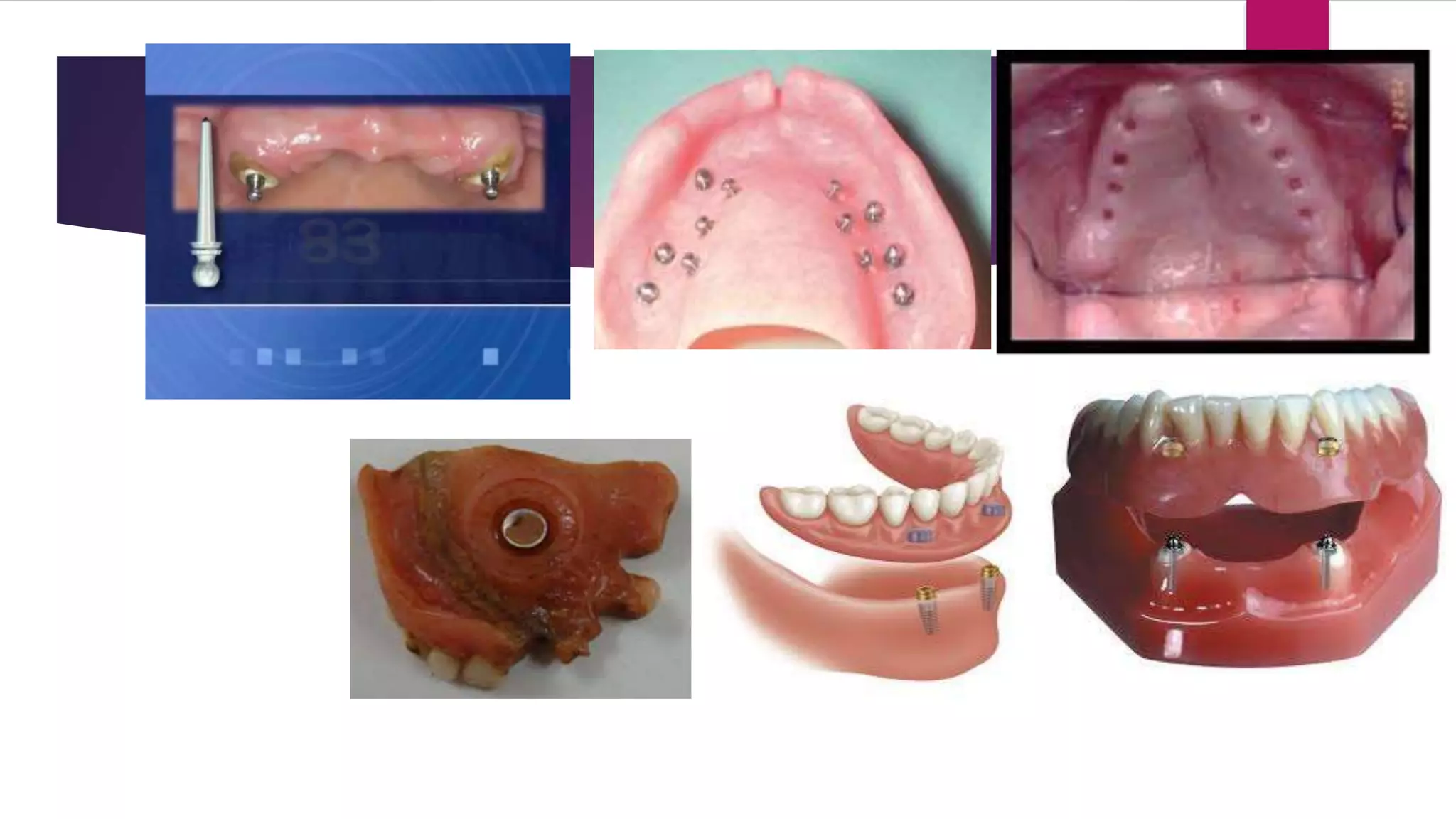

This document discusses principles of retention, support and stability in complete dentures. It defines retention as the ability of a denture to resist displacement when removed from the mouth. Primary retention involves physical forces like adhesion, cohesion, surface tension and atmospheric pressure between the denture, saliva and mucosa. Mechanical retention adds modifications to the denture like undercuts or attachments. Stability is the ability to resist horizontal or rotational forces, influenced by factors like ridge size and quality. Support is resistance to vertical displacement, provided by areas like the hard palate, tuberosities and residual ridges.

























































![Apporach to lung biopsy [Auto-saved].pptx latest](https://cdn.slidesharecdn.com/ss_thumbnails/apporachtolungbiopsyauto-saved-251211225655-93258539-thumbnail.jpg?width=640&height=640&fit=bounds)















