Download as PDF, PPTX







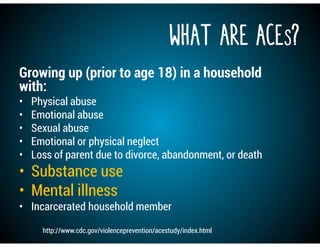
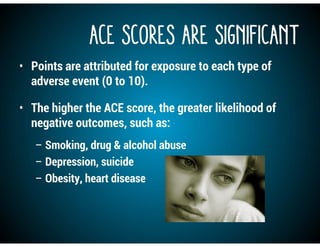
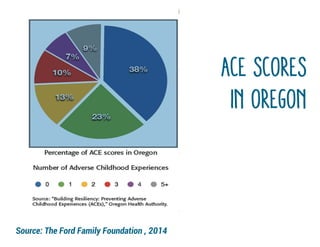
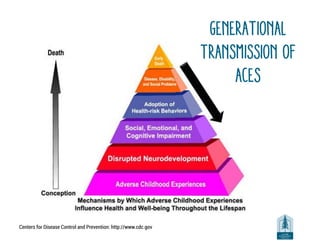
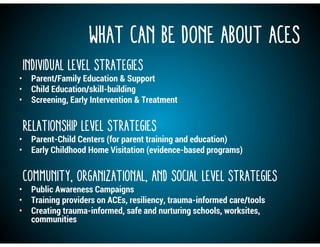


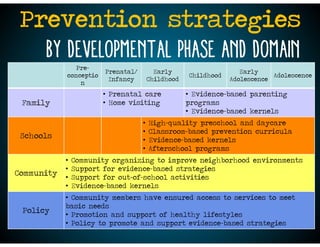


The document discusses substance abuse issues in Lane County, highlighting common risk factors like adverse childhood experiences, and protective factors that can help prevent problems. It provides an overview of current prevention efforts and strategies across different developmental phases, emphasizing building resilience and facilitating healing from trauma through family, school, community and policy supports.































































































