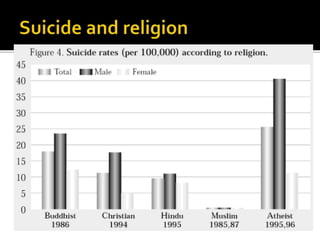
This document discusses suicide prevention and intervention. It begins with an overview of global suicide statistics and risk factors. Common risk factors include mental illness, substance abuse, relationship or financial problems, and physical/sexual abuse. The document then outlines common warning signs like withdrawing from others, feelings of hopelessness, and making plans or notes. It discusses prevalent methods like hanging, poisoning, and firearms. The document concludes with strategies for prevention, like restricting access to lethal means and improving social support systems and healthcare to address mental health issues.



















![Tdv 5 minute overview[1]](https://cdn.slidesharecdn.com/ss_thumbnails/tdv5minuteoverview1-120710205048-phpapp02-thumbnail.jpg?width=640&height=640&fit=bounds)















































