Pregnancy places an additional burden on the heart due to significant hemodynamic changes. The incidence of heart disease during pregnancy has increased due to more women with congenital heart disease surviving to reproductive age. Hemodynamic changes during pregnancy and labor like increased blood volume, heart rate and cardiac output can exaggerate the symptoms of heart conditions. Close monitoring and management of heart conditions and risks is needed before, during and after pregnancy to support a healthy pregnancy outcome.
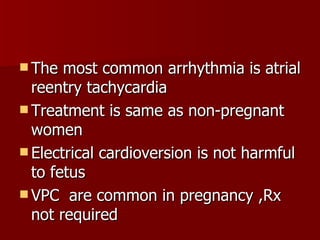
![Physical examination Pulse volume increase JVP-may elevated Apical impulse is more prominent First heart sound appear loud Third heart sound common ESM grade3/6 left sternal edge Continuous murmur[cervical venous hum,mammary suffle] may heard NO DIASTOLIC MURMUR](https://image.slidesharecdn.com/pregnancyandheartdiseaseppt-100518024023-phpapp01/85/Pregnancy-and-Heart-Disease-7-320.jpg)
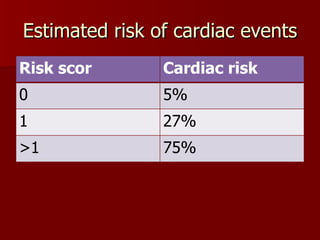
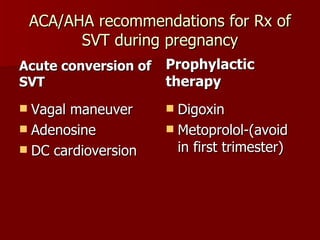
![Risk index Prior cardiac events [HF,TIA,Stroke] or Arrhythmias Baseline NYHA class>2 or cyanosis LVOT obstruction: [MVA<2cm2,AVA<1.5cm2,Peak LVOTpressure gradient>30mmhg] LVEF<40%](https://image.slidesharecdn.com/pregnancyandheartdiseaseppt-100518024023-phpapp01/85/Pregnancy-and-Heart-Disease-9-320.jpg)
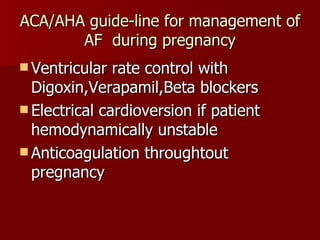
![Moderate risk of mortality [5-15%] NYHA class III and IV Mitral stenosis Severe aortic stenosis Marfan syndrome with normal aorta Uncomplicated coarctation of aorta Past h/o myocardial infarction](https://image.slidesharecdn.com/pregnancyandheartdiseaseppt-100518024023-phpapp01/85/Pregnancy-and-Heart-Disease-13-320.jpg)
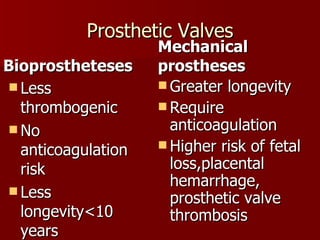
![Highrisk of mortality[25-50%] Eissenmenger’s syndrome Pulmonary hypertension Marfan syndrome with abnormal aorta Peripartum cardiomyopathy](https://image.slidesharecdn.com/pregnancyandheartdiseaseppt-100518024023-phpapp01/85/Pregnancy-and-Heart-Disease-14-320.jpg)






































![Cardiovascular disease students [compatibility mode]](https://cdn.slidesharecdn.com/ss_thumbnails/cardiovasculardisease-studentscompatibilitymode-130509054709-phpapp02-thumbnail.jpg?width=640&height=640&fit=bounds)































































