Download as PDF, PPTX


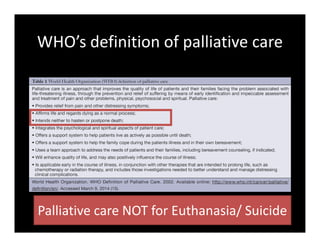
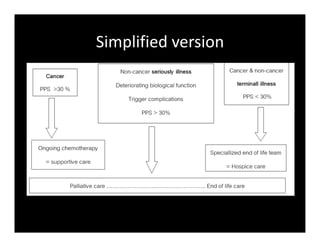
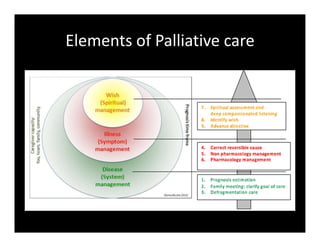
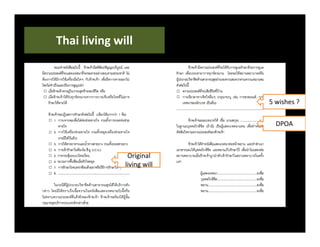
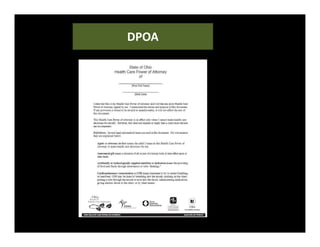
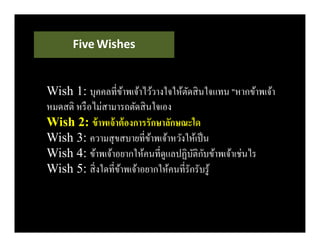
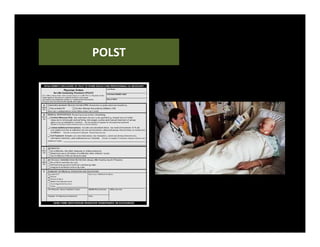



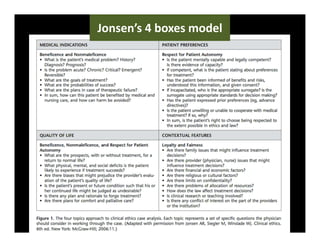
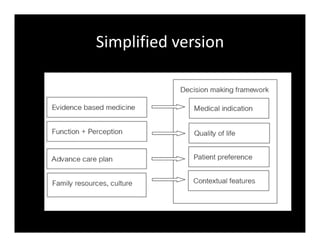
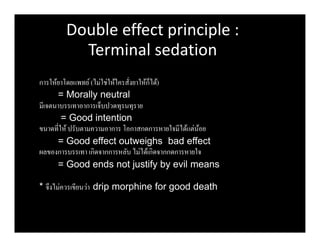

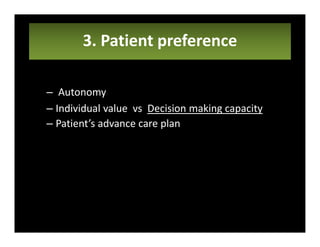
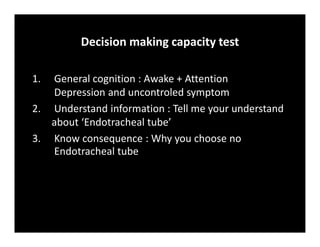
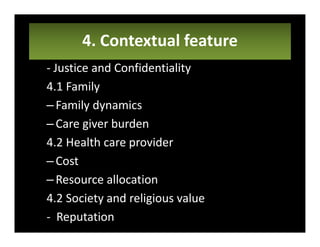


1. Palliative care focuses on relieving suffering through a holistic approach addressing the patient's physical, psychological, and spiritual needs using a 3S framework of system, symptom, and spiritual care. 2. Advance care planning documents a patient's values and preferences for end-of-life care through a "wish" or goal of care and a living will or procedures they do/do not consent to, optionally designating a healthcare proxy. 3. Medical ethical dilemmas are addressed through a 4 box model considering medical indication, quality of life, patient preference, and contextual factors to guide decision making in palliative care.










































































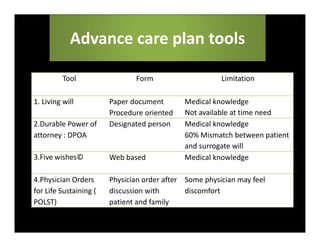
![Hypothalamus short ppt by Dr. Neha [PT].pptx](https://cdn.slidesharecdn.com/ss_thumbnails/hypothalamusbydr-260124145759-b9f94a93-thumbnail.jpg?width=640&height=640&fit=bounds)


