Introduction
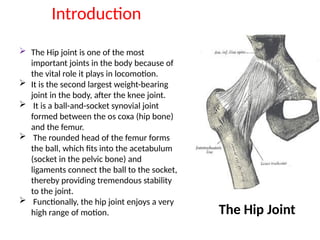
The Hipjoint is one of the most
important joints in the body because of
the vital role it plays in locomotion.
It is the second largest weight-bearing
joint in the body, after the knee joint.
It is a ball-and-socket synovial joint
formed between the os coxa (hip bone)
and the femur.
The rounded head of the femur forms
the ball, which fits into the acetabulum
(socket in the pelvic bone) and
ligaments connect the ball to the socket,
thereby providing tremendous stability
to the joint.
Functionally, the hip joint enjoys a very
high range of motion. The Hip Joint
3.
All ofthe various components of the hip
mechanism assist in the mobility of the joint.
Damage to any single component can
negatively affect range of motion and ability to
bear weight on the joint.
In hip injury, as with other traumatic
presentations, age distribution is bimodal with
high-energy trauma in the younger population
and potentially trivial mechanisms of injury in
the older population, e.g. a simple fall.
4.
Subjective Examination
Patient Intake
Thefirst step during the examination is the patient interview, during
which the clinician gets a description of the presenting symptoms
from the patient.
Research suggests patient history plays a vital role in the differential
diagnosis of hip pain and, in some cases, can be superior to objective
tests and measures.
Taking the history is a vital component of the subjective examination
as it helps the clinician develop a hypothesis about the mechanism of
injury, type of the injured structures and extent of the injury or
damage.
5.
Details like thelocation of the pain, nature of the pain, 24-hour
pattern of the pain, activities that trigger the pain, pain aggravating
and relieving factors etc., are gotten from the patient during the
interview.
According to new systematic review published in the Archives of
Physical Medicine and Rehabilitation, thigh/groin pain and constant
back/buttock pain are better indicators of hip OA than stand-alone
tests and reported hip crepitus is a strong indicator of intra-articular
hip pathology.
The patient's past medical history, as well as their social/family history
is also important as this helps the clinician rule out hereditary
conditions. Any surgical histories that are specific to the hip region is
also vital, for example, a patient who had a hip joint replacement
surgery and is currently complaining of pain at the hip joint.
6.
The patient's drughistory and current medications they are on should
also be documented as well as any allergies they might have.
The effects of the condition on the patient' functional status and
Activities of Daily Living (ADLs) should be well assessed and
documented.
In the elderly it is also worth considering whether a fall was the result
of a simple trip, or secondary to another reason, e.g. seizure,
cardiovascular trigger, stroke or loss of consciousness. Relevant
assessment of the cardiovascular or neurological system may be
required with additional tests, e.g. ECG, CT brain.
7.
Special Considerations
Red Flags[3]
Sudden onset of pain.
A history of trauma
Any swelling
Any deformity
An inability to bear weight
Any lumps or bumps felt in the groin
Night pain
Any noticeable groin pulsations
Constipation or vomiting
Haematuria
Fever
8.
Lower limbneurological symptoms - weakness, numbness or tingling
History of steroid use
Testicular swelling
Night sweats, unintentional weight loss, appetite loss
History of malignancy
High-risk sexual activity
Other Flags
It is also important to screen for
other (yellow, orange, blue and black) flags as these may interfere with
physiotherapy interventions.
10.
Investigations
The firstinvestigation of choice in a patient with hip pain following trauma is a hip x-
ray.
This will be an AP radiograph of the pelvis and a lateral radiograph of the painful
hip.
Fractures are not always identified on initial x-ray imaging. If there is a clinical
concern for a hip fracture, but the x-ray is normal, further imaging is required.
Both CT and MRI can be used to look for a radiographically occult fracture - MRI is
more sensitive, but CT is usually easier to organize and in many institutions is the
second-line investigation of choice.
In complex fractures, CT can be helpful to get additional preoperative information
that can be used to plan surgery and aid discussion about consent and prognosis.
It is also worthwhile considering that interpretation of a hip x-ray will be
complicated in the elderly by the present of other conditions, e.g. secondary
osteoarthritis.
11.
Objective Examination
Observation
Upon conclusionof the patient interview, the clinician proceeds to the objective examination. A
Pain VAS is administered to determine the patient's baseline pain level and then the examiner
observes and documents the following:
✂ Bony deformity / Bony alignment
1. Gait pattern: There are several types of abnormal gait patterns associated with hip
pathologies which the clinician needs to look out for such as Antalgic gait, Trendelenburg
gait, Arthrogenic gait and Lurching gait.
2. Weight Bearing
3. Balance and Posture
4. In Standing: Lumbar spine, Level of iliac crests (To rule out pelvic/SIJ dysfunction)
5. Lying Supine: Leg length (apparent and real leg lengths), External rotation of leg.
✂ Colour changes e.g. bruising, inflammation, infection, rash.
✂ Muscle wasting, muscle spasm and muscle bulk.
✂ Swelling, scarring, skin changes (wounds).
Neurologic Assessment
ManualMuscle Testing: The strength of the muscle groups
surrounding the hip joint, namely the hip extensors, flexors,
abductors, adductors, internal and external rotators should be
graded and documented.
Straight Leg Raise
Dermatome Testing
Skin sensation test
15.
Movement Testing
Theavailable ranges of motion at the hip joint (Active and
Passive) are measured using a goniometer and documented.
These measurements serve as baseline readings and help
determine if the intervention is yielding results.
17.
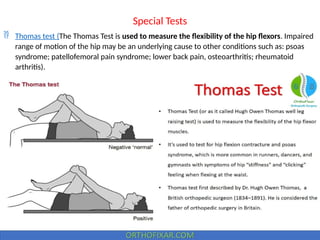
Special Tests
Thomastest (The Thomas Test is used to measure the flexibility of the hip flexors. Impaired
range of motion of the hip may be an underlying cause to other conditions such as: psoas
syndrome; patellofemoral pain syndrome; lower back pain, osteoarthritis; rheumatoid
arthritis).
18.
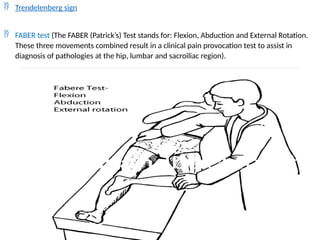
Trendelenberg sign
FABER test (The FABER (Patrick’s) Test stands for: Flexion, Abduction and External Rotation.
These three movements combined result in a clinical pain provocation test to assist in
diagnosis of pathologies at the hip, lumbar and sacroiliac region).
19.
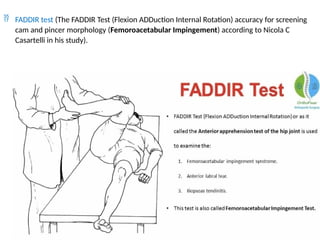
FADDIR test(The FADDIR Test (Flexion ADDuction Internal Rotation) accuracy for screening
cam and pincer morphology (Femoroacetabular Impingement) according to Nicola C
Casartelli in his study).
20.
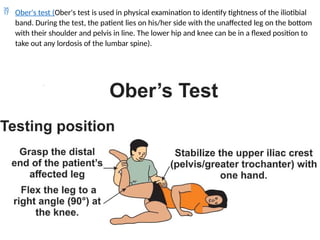
Ober's test(Ober's test is used in physical examination to identify tightness of the iliotibial
band. During the test, the patient lies on his/her side with the unaffected leg on the bottom
with their shoulder and pelvis in line. The lower hip and knee can be in a flexed position to
take out any lordosis of the lumbar spine).
21.
Log rolltest (The log roll test assesses for pathology within the hip joint, and can be used to
isolate the patient's pathology to the hip as opposed to outside of the hip joint.
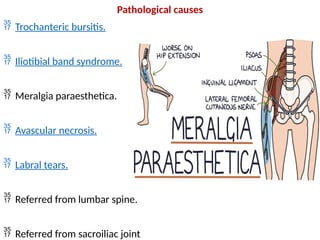
Malignant causes
Osteosarcoma.
Metastatic disease such as prostate cancer or pelvic tumours.
Miscellaneous
Renal calculus (loin to groin pain).
Iliopsoas abscess.

![Special Considerations
Red Flags[3]
Sudden onset of pain.
A history of trauma
Any swelling
Any deformity
An inability to bear weight
Any lumps or bumps felt in the groin
Night pain
Any noticeable groin pulsations
Constipation or vomiting
Haematuria
Fever](https://image.slidesharecdn.com/random-250309075050-e8730ddd/85/pptx-7-320.jpg)























































![Hypothalamus short ppt by Dr. Neha [PT].pptx](https://cdn.slidesharecdn.com/ss_thumbnails/hypothalamusbydr-260124145759-b9f94a93-thumbnail.jpg?width=640&height=640&fit=bounds)















