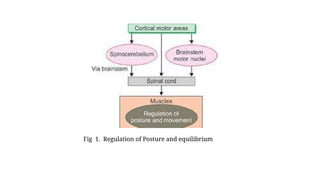
POSTURE AND EQUILIBRIUM
Dr.E. Muralinath, Dr. M. Guruprasad, Dr. K.
Sravani Pragna, Dr. C. Kalyan, Dr. P. Manjari, Dr. D.
Kusumalatha, Dr. K. Sridevi , Dr. Ch. Ramya Sudha
and R. Gnana Lahari
2.
• DEFINITION
• Subconsciousadjustment of tone in different muscles in relation to every movement is termed as
the posture.
• BASIC PHENOMENA OF POSTURE
• Basic phenomena for maintenance of posture are muscle tone and stretch reflex.
• MUSCLE TONE
• Definition
• Muscle tone is narrated as the state of continuous and passive partial contraction of muscle along
with certain vigor and tension.
• 2) It is also otherwise known as tonus. It is also narrated as
• resistance offered by the muscle to stretch.
•
3.
• Significance ofMuscle Tone
• Muscle tone plays an important role regarding the maintenance of posture.
• Change in muscle tone enables movement of different parts of the body.
• Muscle tone is observed in all the skeletal muscles.
• Whatever it may be, tone is more in antigravity muscles namely extensors of lower limb, trunk
muscles and neck muscles.
•
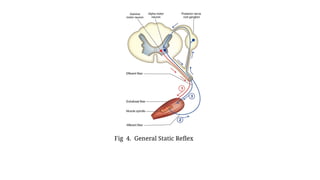
• Development of Muscle Tone
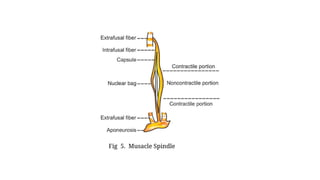
• A)Gamma motor neurons and muscle spindle are responsible for the development and
maintenance of muscle tone.
•
•
4.
• Sequence ofevents
• 1. Impulses from the gamma motor neurons createcontraction of end portions of intrafusal fibers
(stimulus)
• 2. This stretches and activates the central portion of the intrafusal fibers, which initiates the reflex action
particularly for development of muscle tone with the help of discharge of the
• impulses
• Supraspinal facilitatory centers
• Supraspinal centers, which enhance the muscle tone: 1. Motor area 4 in cerebral cortex
• 2. Cerebellum
• 3. Descending facilitatory reticular system
• 4. Red nucleus
• 5. Vestibular nucleus.
•
5.
• Supraspinal inhibitorycenters
• Supraspinal centers, which reduce the muscle tone:
• 1. Suppressor areas of cerebral cortex
• 2. Basal ganglia
6.
• Role ofmotor area of cerebral cortex – coactivation
• Motor area of cerebral cortex influences especially the activity of lower motor neurons by sending
motor impulses through the pyramidal tract fibers.
•
• 5. Alpha motor neurons in turn, send impulses to extrafusal fibers of the muscle through spinal
nerve fibers (efferent fibers)
•
• 6. These impulses cause partial contraction of the muscle fibers leading to development of muscle
tone (response). If the frequency of discharge from gamma motor neurons enhances, the activity of
muscle spindle Is also enhanced and muscle tone also enhances. An activation of gamma motor
neurons enhances the muscle tone. Lesion in gamma motor neurons results in loss of tone in
muscles.
7.
• Even thoughthe muscle tone is developed by discharges from gamma motor neurons, it is regulated in a
continuous manner particularly from cerebral cortex activate both α
motor neurons and γ
motor neurons
simultaneously.
• This type of Simultaneous activation is termed as coactivation. It is also called α-γ coactivation.
•
• Role of cerebellum and basal ganglia
• It is interesting to find that cerebellum and basal ganglia impact the muscle tone without sending direct
fibers to γ
motor neurons.
• These parts of brain impact the muscle tone indirectly through brainstem centers.
• Role of brainstem centers
• Brainstem centers which impact the γ
motor neurons are in reticular formation, red nucleus and vestibular
nucleus.
• These centers modulate the discharge especially from γ
motor neurons by obtaining signals from
cerebral cortex, cerebellum and basal ganglia.
8.
• STRETCH REFLEX
•Basic reflex participated in maintenance of posture is the stretch reflex.
• This reflex is normally observed and serves especially to regulate the body in an upright position.
• Such reflexes are, therefore more pronounced in extensor muscles.
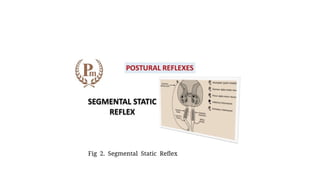
• POSTURAL REFLEXES
• A)Postural reflexes are the reflexes that play an important role regarding maintenance of posture.
• B)Afferent impulses for the maintenance of posture arise from proprioceptors,
• C)vestibular apparatus and retina of e
9.
•
• CLASSIFICATION OFPOSTURAL REFLEXES
• Postural reflexes are generally categorized into two groups:
• A. Static reflexes
• B. Statokinetic reflexes.
• STATIC REFLEXES
• Static reflexes are the postural reflexes that regulate posture at rest. Static reflexes are of four types:
• I. General static reflexes or righting reflexes
• II. Local static reflexes or supporting reflexes
• III. Segmental static reflexes
• IV. Statotonic or attitudinal reflexes.
• . General Static Reflexes or Righting Reflexes
• A)General static reflexes are otherwise known as righting reflexes because these reflexes assist regarding maintenance of an upright position of the body.
• B) Righting reflexes assist to govern the orientation of the head in space, position of the head in relation to the body and appropriate adjustment of the limbs
and eyes in relation to the position of the head, so that upright position of the body is regulated.
• C)If a cat, held with its back downwards, is permitted to fall through the air, it lands upon its paws, with the head and body getting the normal attitude in a flash.
• D) A fish resists any attempt to turn it from its normal position and if it is placed in water upon its back, it flips almost in an instant manner into the normal
swimming position.
•
10.
•
• Righting reflexesare categorized into five types:
• 1. Labyrinthine righting reflexes acting on the neck muscles
• 2. Neck righting reflexes acting on the body
• 3. Body righting reflexes acting on the head
• 4. Body righting reflexes acting on the body
• 5. Optical righting reflexes
• First four reflexes are demonstrated in an easy manner on a thalamic animal or a normal animal, which is blindfolded.
• 1. Labyrinthine righting reflexes acting on the neck muscles
• A)If a thalamic animal (rabbit) is suspended by holding at the pelvic region, its head turns up, until it regains its normal position.
• B)It is because of reflexes arising from labyrinth, the sensory organ associated with equilibrium of head, in regard to the position of the body.
• C)Turning the body of animal through air into different positions is followed by compensatory movements of the head.
•
• Neck righting reflexes acting on the body
• It is observed that during labyrinthine righting reflexes, the head raises up to normal position.
• ii)It is because of the contraction of neck muscles. Now, the contraction of neck muscles gives rise to proprioceptive impulses, which show their
actions on the body and rotate the body in relation to position of head.
• iii)This reflexis well observed, if the animal is laid down in resting position upon its side on a table.
11.
• A)Labyrinthine rightingreflexes are not the only reflexes acting on neck muscles to create rotation of head.
• B)If the animal is laid down upon its side on a table, the unequal distribution of pressure on that particular side of the body
activates exteroceptors on the skin.
• C)Impulses thus produced by exteroceptors, act on neck muscles and rotate the head.
•
• Body righting reflexes acting on the body
• If the same animal is laid down on the table on its side, with head held down to table, to remove labyrinthine and neck righting
reflexes, the body attempts to right itself by raising the lower parts.
• It is because of the impulses from exteroceptors on that side of body acting on the body itself.
•
• 5. Optical righting reflexes
• A)Optical righting reflexes happened with the help of the retinal impulses.
• B)Center for optical righting reflexes is in the occipital lobe of cerebral cortex.
• C)So, these reflexes are absent in thalamic animal. Optical righting reflexes assistto correct the position of the body or head with
the help of sight. It is proved especially in labyrinthectomized animal.
• D)If such an animal is suspended, it rotates its head to normal position with the help of sight.
12.
Summary of rightingreflexes
• Following are the sequential events of righting reflexes:
• i. If the animal is placed upon its back, labyrinthine reflexes acting upon neck muscles turn the head into its normal position in
space, in relation to body
• ii. Proprioceptive reflexes of neck muscles then bring the body into its normal position regarding position of head
• iii. If resting upon a rigid support, these reflexes are reinforced by the body righting reflexes on the head as well as on the body
• iv. If the animal happens to be a labyrinthectomized one, then it makes an effort to recover its upright position as a result of
operation of the optical righting reaction. If the optical righting reflexes are eliminated by covering the eyes, the righting
capability is lost.
• v)Optical righting reflexes are also demonstrated in 3 or 4 weeks old baby. When laid down on belly, i.e. prone position, the
baby tries to raise the head to a vertical
• position.
• vi)Centers for righting reflexes
• Centers for the first four righting reflexes are in red nucleus located in midbrain. Center for optical righting reflexes is in the
occipital lobe of cerebral cortex.
•
13.
• II. LocalStatic Reflexes or Supporting Reflexes
• Local static reflexes or supporting reactions assist the body in different positions against gravity and also protect the limbs particularly against
hyperextension or hyperflexion.
• Supporting reactions are categorized into two types:
• 1. Positive supporting reflexes
• 2. Negative supporting reflexes.
• 1. Positive supporting reflexes
• 1.Positive supporting reflexes:-
• A)These reflexes are the reactions, which assist to fix the joints and make the limbs rigid such as pillars, so that limbs can support the weight of
the body against gravity.
• B)It is brought about by the simultaneous reflex contractions of both extensor and flexor muscles and other opposing muscles.
• C) The impulses for these reflexes arise from proprioceptors observed in the muscles, joints and tendons and the exteroceptors, especially
pressure receptors observed in deeper layers of the skin of sole.
• D)While standing, the positive supporting reflexes are produced in the following manner: If an animal stands on its limbs, the pressure of the
animal’s paw upon the ground produces proprioceptive impulses from flexor and extensor muscles of the limbs, especially in terminal segments
of the limbs like digits, ankle or wrist.
• ii. Excessive extension at the joints is checked or guarded by the myotatic reflexes setting up in the flexor muscles. When the flexor muscles
are simultaneously contracting, extensor muscles cannot be stretched beyond the physiological limits. Similarly, over activity of the flexor
muscles is stopped by the stretch reflexes developed in the extensor muscles.
14.
• iii. Impulsesarise even from exteroceptors while standing, if the sole remains in contact
• with the ground. It causes an activation of the pressure receptors, which are observed in
• deeper layers of the skin. These impulses from pressure receptors reinforce the rigidity of the
• limbs occurred by the proprioceptive impulses
• 2. Negative supporting reflexes
• A)Relaxation of the muscles and unfixing of the joints enable the limbs to flex and move to a new position.
• B)It is also otherwise known as negative supporting reaction.
• C)It is brought about by raising the leg off the ground and plantar flexion of toes and ankle.
• D) If the leg is lifted off the ground, the exteroceptive impulses are prevented.
• E)When the toes and ankle joints are plantar flexed, the stretch stimulus for the plantar muscles is prevented.
• The positive and negative supporting reactions are demonstrated well on a decorticate animal. The centers
for the supporting reflexes are situated in the spinal cord.
•
15.
• III. SegmentalStatic Reflexes
• 1)Segmental static reflexes are very responsible for walking.
• 2) During walking, in one leg, the flexors are active and the extensors are not activated.
• 3)On the opposite leg, the flexors are inhibited and extensors are active.
• 4)Thus, the flexors and extensors of the same limb are not active in a simultaneous manner. It is also termed as crossed extensor reflex.
• 5)It is because of the reciprocal inhibition and the neural mechanism responsible for this reflex is termed as Sherrington reciprocal innervation.
• IV. Stat tonic or Attitudinal Reflexes
• Statotonic or attitudinal reflexes are developed according to the attitude of the body and are of two types:
• 1. Tonic labyrinthine and neck reflexes acting on the limbs
• 2. Labyrinthine and neck reflexes acting on the eyes.
•
• 1. Tonic labyrinthine and neck reflexes acting on the limbs
• A)Tonic labyrinthine and neck reflexes reduce or enhance the tone of the skeletal muscles of the limbs in accordance to the attitude or position of the
head.
• B) These reflexes are best studied in decerebrate animal.
• C)The proprioceptors associated with these reflexes are in the labyrinthine apparatus. D)Whenever the position of the head is altered, the receptors
present in the labyrinth are stimulated and proiduce impulses.
• E)The impulses are also generated from the neck muscles because of alteration of position of the head.
16.
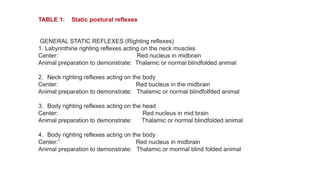
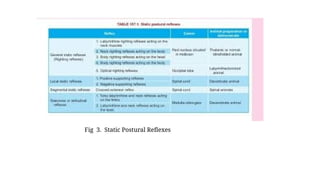
TABLE 1: Staticpostural reflexes
Reflex
Center
GENERAL STATIC REFLEXES (Righting reflexes)
1. Labyrinthine righting reflexes acting on the neck muscles
Center: Red nucleus in midbrain
Animal preparation to demonstrate: Thalamic or normal blindfolded animal
2. Neck righting reflexes acting on the body
Center: Red bucleus in the midbrain
Animal preparation to demonstrate: Thalamic or normal blindfolfded animal
3. Body righting reflexes acting on the head
Center: Red nucleus in mid brain
Animal preparation to demonstrate: Thalamic or normal blindfolded animal
4. Body righting reflexes acting on the body
Center:” Red nucleus in midbrain
Animal preparation to demonstrate: Thalamic or mormal blind folded animal
17.
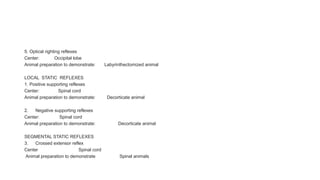
5. Optical rightingreflexes
Center: Occipital lobe
Animal preparation to demonstrate: Labyrinthectomized animal
LOCAL STATIC REFLEXES
1. Positive supporting reflexes
Center: Spinal cord
Animal preparation to demonstrate: Decorticate animal
2. Negative supporting reflexes
Center: Spinal cord
Animal preparation to demonstrate: Decorticate animal
SEGMENTAL STATIC REFLEXES
3. Crossed extensor reflex
Center Spinal cord
Animal preparation to demonstrate Spinal animals
18.
•
•
• STATOTONIC ORATTITUDINAL REFLEXES
• 1. Tonic labyrinthine and neck reflexes acting
• on the limbs
• Center: Medulla Oblongata
• Medulla oblongata
• Animal preparation to demonstrate: Decerebrate animal llllj
•
• 2. Labyrinthine and neck reflexes acting on
• the eyes
• Center: Medulla Oblongata
• Animal preparation to demonstrate: Decorticate animal
The impulses from labyrinth create the same effect on all the four limbs.
• But the impulses from neck muscles cause opposite effects in the forelimbs and hind limbs.
• The labyrinthine reflexes are specifically effective on extensor muscles.
• If the head is dorsiflexed, all the four limbs are extended maximally and if the head is ventriflexed, all the four limbs are flexed.
• In a labyrinthectomized animal where only neck reflexes are operated, during dorsiflexion of the head, there is extension of the forelimbs and flexion of the hind limbs.
• The ventriflexion of the head leads to flexion of the forelimbs and extension of the hind limbs.
• The importance of these reflexes is understood well, while observing the movements during change in the attitude of a normal animal.
•
19.
• STATOKINETIC REFLEXES
•Statokinetic reflexes are the postural reflexes that regulate posture during movement. B)These
reflexes are associated with both angular (rotatory) and linear (progressive) movements.
• C) The vestibular apparatus is responsible for these reflexes. So, it is responsiblel to
• study the structure and functions of vestibular apparatus to understand the statokinetic reflexes.
•
•
REFERENCES
• REFERENCES:-
• PalakurthiB, Burugupally SP. Postural Instability in Parkinson's Disease: A Review. Brain Sci. 2019 Sep 18;9(9) [PMC free article] [PubMed]
• 2.
• Koller WC, Glatt S, Vetere-Overfield B, Hassanein R. Falls and Parkinson's disease. Clin Neuropharmacol. 1989 Apr;12(2):98-105. [PubMed]
• 3.
• Rinalduzzi S, Trompetto C, Marinelli L, Alibardi A, Missori P, Fattapposta F, Pierelli F, Currà A. Balance dysfunction in Parkinson's disease. Biomed
Res Int. 2015;2015:434683. [PMC free article] [PubMed]
• 4.
• Allen NE, Schwarzel AK, Canning CG. Recurrent falls in Parkinson's disease: a systematic review. Parkinsons Dis. 2013;2013:906274. [
PMC free article] [PubMed]
• 5.
• Grimbergen YA, Munneke M, Bloem BR. Falls in Parkinson's disease. Curr Opin Neurol. 2004 Aug;17(4):405-15. [PubMed]
• 6.
• Salzman B. Gait and balance disorders in older adults. Am Fam Physician. 2010 Jul 01;82(1):61-8. [PubMed]
• 7.
• Gnädinger M, Mellinghoff HU, Kaelin-Lang A. Parkinson's disease and the bones. Swiss Med Wkly. 2011;141:w13154. [PubMed]
• 8.
• Baron EM, Young WF. Cervical spondylotic myelopathy: a brief review of its pathophysiology, clinical course, and diagnosis. Neurosurgery. 2007
Jan;60(1 Supp1 1):S35-41. [PubMed]
27.
• 9.
• DyckPJ, Dyck PJ, Grant IA, Fealey RD. Ten steps in characterizing and diagnosing patients with peripheral neuropathy.
Neurology. 1996 Jul;47(1):10-7. [PubMed]
• 10.
• Knutsson E, Lying-Tunell U. Gait apraxia in normal-pressure hydrocephalus: patterns of movement and muscle activation.
Neurology. 1985 Feb;35(2):155-60. [PubMed]
• 11.
• Peckham EL, Hallett M. Psychogenic movement disorders. Neurol Clin. 2009 Aug;27(3):801-19, vii. [PMC free article] [PubMed]
• 12.
• Muncie HL, Sirmans SM, James E. Dizziness: Approach to Evaluation and Management. Am Fam Physician. 2017 Feb
01;95(3):154-162. [PubMed]
• 13.
• Kim SD, Allen NE, Canning CG, Fung VS. Postural instability in patients with Parkinson's disease. Epidemiology, pathophysiology
and management. CNS Drugs. 2013 Feb;27(2):97-112. [PubMed]
• 14.
• Orr R. Contribution of muscle weakness to postural instability in the elderly. A systematic review. Eur J Phys Rehabil Med. 2010
Jun;46(2):183-220. [PubMed]
28.
• 15.
• MüllerMLTM, Marusic U, van Emde Boas M, Weiss D, Bohnen NI. Treatment options for postural instability and gait
difficulties in Parkinson's disease. Expert Rev Neurother. 2019 Dec;19(12):1229-1251. [PubMed]
• 16.
• Litvan I. Update on progressive supranuclear palsy. Curr Neurol Neurosci Rep. 2004 Jul;4(4):296-302. [PubMed]
• 17.
• Bloem BR. Postural instability in Parkinson's disease. Clin Neurol Neurosurg. 1992;94 Suppl:S41-5. [PubMed]
• 18.
• Grimbergen YA, Langston JW, Roos RA, Bloem BR. Postural instability in Parkinson's disease: the adrenergic
hypothesis and the locus coeruleus. Expert Rev Neurother. 2009 Feb;9(2):279-90. [PubMed]
• 19.
• Gelb DJ, Oliver E, Gilman S. Diagnostic criteria for Parkinson disease. Arch Neurol. 1999 Jan;56(1):33-9. [PubMed]
• 20.
• Hillen ME, Wagner ML, Sage JI. "Subclinical" orthostatic hypotension is associated with dizziness in elderly patients
with Parkinson disease. Arch Phys Med Rehabil. 1996 Jul;77(7):710-2. [PubMed]









![REFERENCES
• REFERENCES:-
• Palakurthi B, Burugupally SP. Postural Instability in Parkinson's Disease: A Review. Brain Sci. 2019 Sep 18;9(9) [PMC free article] [PubMed]
• 2.
• Koller WC, Glatt S, Vetere-Overfield B, Hassanein R. Falls and Parkinson's disease. Clin Neuropharmacol. 1989 Apr;12(2):98-105. [PubMed]
• 3.
• Rinalduzzi S, Trompetto C, Marinelli L, Alibardi A, Missori P, Fattapposta F, Pierelli F, Currà A. Balance dysfunction in Parkinson's disease. Biomed
Res Int. 2015;2015:434683. [PMC free article] [PubMed]
• 4.
• Allen NE, Schwarzel AK, Canning CG. Recurrent falls in Parkinson's disease: a systematic review. Parkinsons Dis. 2013;2013:906274. [
PMC free article] [PubMed]
• 5.
• Grimbergen YA, Munneke M, Bloem BR. Falls in Parkinson's disease. Curr Opin Neurol. 2004 Aug;17(4):405-15. [PubMed]
• 6.
• Salzman B. Gait and balance disorders in older adults. Am Fam Physician. 2010 Jul 01;82(1):61-8. [PubMed]
• 7.
• Gnädinger M, Mellinghoff HU, Kaelin-Lang A. Parkinson's disease and the bones. Swiss Med Wkly. 2011;141:w13154. [PubMed]
• 8.
• Baron EM, Young WF. Cervical spondylotic myelopathy: a brief review of its pathophysiology, clinical course, and diagnosis. Neurosurgery. 2007
Jan;60(1 Supp1 1):S35-41. [PubMed]](https://image.slidesharecdn.com/postureequllibrium-250716045433-82c73bd6/85/Posture-Equilibrium_________locomotion-26-320.jpg)
![• 9.
• Dyck PJ, Dyck PJ, Grant IA, Fealey RD. Ten steps in characterizing and diagnosing patients with peripheral neuropathy.
Neurology. 1996 Jul;47(1):10-7. [PubMed]
• 10.
• Knutsson E, Lying-Tunell U. Gait apraxia in normal-pressure hydrocephalus: patterns of movement and muscle activation.
Neurology. 1985 Feb;35(2):155-60. [PubMed]
• 11.
• Peckham EL, Hallett M. Psychogenic movement disorders. Neurol Clin. 2009 Aug;27(3):801-19, vii. [PMC free article] [PubMed]
• 12.
• Muncie HL, Sirmans SM, James E. Dizziness: Approach to Evaluation and Management. Am Fam Physician. 2017 Feb
01;95(3):154-162. [PubMed]
• 13.
• Kim SD, Allen NE, Canning CG, Fung VS. Postural instability in patients with Parkinson's disease. Epidemiology, pathophysiology
and management. CNS Drugs. 2013 Feb;27(2):97-112. [PubMed]
• 14.
• Orr R. Contribution of muscle weakness to postural instability in the elderly. A systematic review. Eur J Phys Rehabil Med. 2010
Jun;46(2):183-220. [PubMed]](https://image.slidesharecdn.com/postureequllibrium-250716045433-82c73bd6/85/Posture-Equilibrium_________locomotion-27-320.jpg)
![• 15.
• Müller MLTM, Marusic U, van Emde Boas M, Weiss D, Bohnen NI. Treatment options for postural instability and gait
difficulties in Parkinson's disease. Expert Rev Neurother. 2019 Dec;19(12):1229-1251. [PubMed]
• 16.
• Litvan I. Update on progressive supranuclear palsy. Curr Neurol Neurosci Rep. 2004 Jul;4(4):296-302. [PubMed]
• 17.
• Bloem BR. Postural instability in Parkinson's disease. Clin Neurol Neurosurg. 1992;94 Suppl:S41-5. [PubMed]
• 18.
• Grimbergen YA, Langston JW, Roos RA, Bloem BR. Postural instability in Parkinson's disease: the adrenergic
hypothesis and the locus coeruleus. Expert Rev Neurother. 2009 Feb;9(2):279-90. [PubMed]
• 19.
• Gelb DJ, Oliver E, Gilman S. Diagnostic criteria for Parkinson disease. Arch Neurol. 1999 Jan;56(1):33-9. [PubMed]
• 20.
• Hillen ME, Wagner ML, Sage JI. "Subclinical" orthostatic hypotension is associated with dizziness in elderly patients
with Parkinson disease. Arch Phys Med Rehabil. 1996 Jul;77(7):710-2. [PubMed]](https://image.slidesharecdn.com/postureequllibrium-250716045433-82c73bd6/85/Posture-Equilibrium_________locomotion-28-320.jpg)



































































