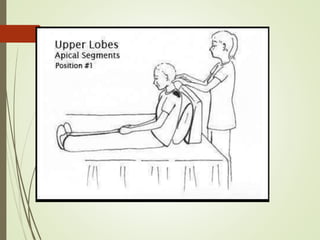
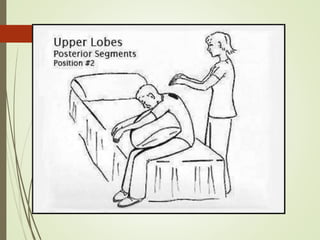
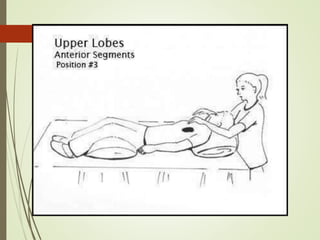
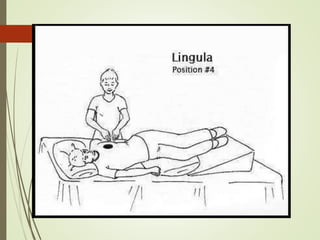
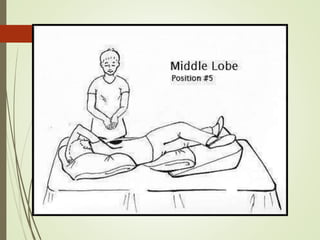
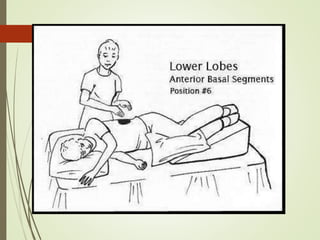
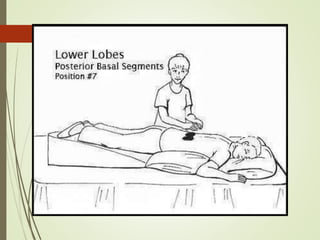
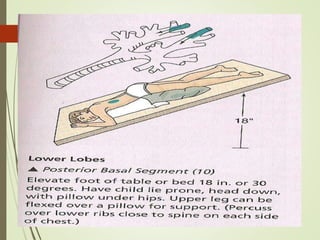
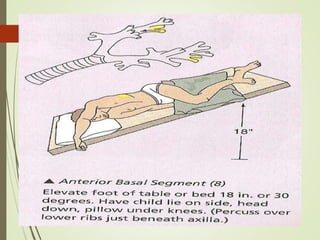
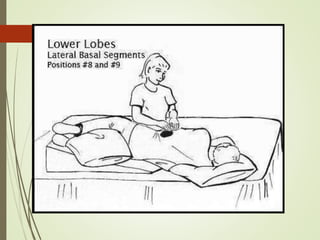
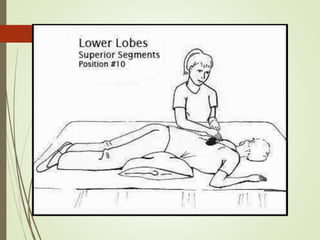
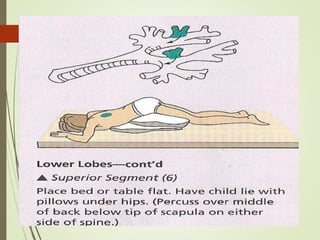
Postural drainage is a technique used to clear secretions from the lungs by positioning the patient in different postures to allow gravity and chest physiotherapy maneuvers to drain secretions. It involves placing patients in positions that target specific lung segments, such as having patients lie on their sides or front to drain the lower lobes. Preparation may include loosening secretions with bronchodilators prior. Manual techniques like percussion, clapping, vibration, and shaking are then applied over involved lung segments during breathing to help dislodge secretions. Postural drainage is effective for conditions with increased mucus production like cystic fibrosis.