Download as PDF, PPTX

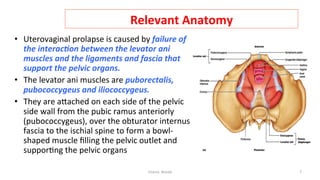
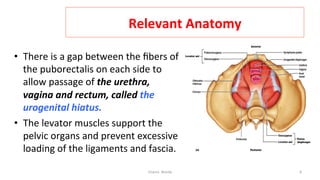
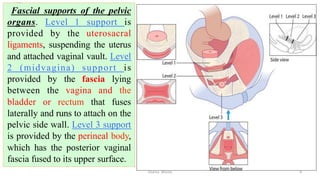
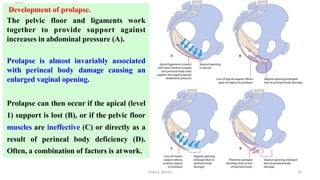
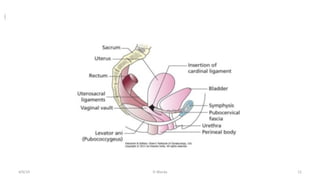
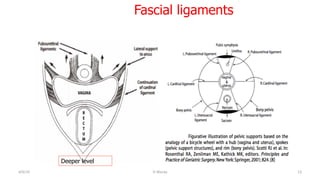
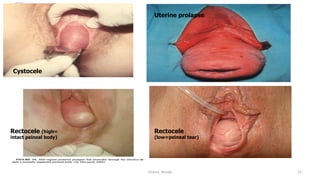

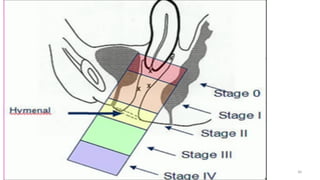


This document provides information on pelvic organ prolapse (POP). It defines POP as the descent of pelvic organs, such as the bladder, rectum or uterus, below their normal position due to distortion of their supportive structures. Symptoms can be direct, such as a vaginal bulge, or indirect due to organ dysfunction. Risk factors include weak pelvic tissues from birth or trauma from childbirth. The levator ani muscles and fascial ligaments normally provide dynamic support against abdominal pressure to prevent prolapse, but damage can occur from childbirth or other causes.







































![SUPPORTS_OF_UTERUS[1] to be continued.pptx](https://cdn.slidesharecdn.com/ss_thumbnails/supportsofuterus1tobecontinued-260110173121-429eaa95-thumbnail.jpg?width=640&height=640&fit=bounds)













































![PERI-PROSTHETIC FRACTURE NAIL-PLATE CONSTRUCT [NPC].pptx](https://cdn.slidesharecdn.com/ss_thumbnails/drarunkumardrmohamedashrafperiprostheticfrasturenail-plateconstructnpc-260209164459-7e9d15a1-thumbnail.jpg?width=640&height=640&fit=bounds)

