Introduction
Polypharmacy isthe concurrent use of multiple
medications - WHO
5 or > 5 medication daily.
Polus = Many (Greek)
Pharmakeia = Use of drugs.
Medications includes Over the counter drugs,
prescription drugs, Traditional / Complementary
medicines.
4.
Prevalence
• It isa Major and growing Global Health issue.
• Due to variations in the structure of Health care delivery
and data collection system of various countries.
• More prevalent in USA and European countries.
• Increase of elderly population of age group > 65 yrs.
• Multimorbidity markedly increases with age and
Prevalence of chronic conditions.
• Results in combined Negative effect on both Physical and
Mental health.
5.
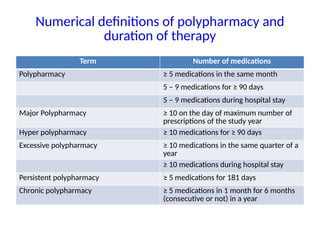
Numerical definitions ofpolypharmacy and
duration of therapy
Term Number of medications
Polypharmacy ≥ 5 medications in the same month
5 – 9 medications for ≥ 90 days
5 – 9 medications during hospital stay
Major Polypharmacy ≥ 10 on the day of maximum number of
prescriptions of the study year
Hyper polypharmacy ≥ 10 medications for ≥ 90 days
Excessive polypharmacy ≥ 10 medications in the same quarter of a
year
≥ 10 medications during hospital stay
Persistent polypharmacy ≥ 5 medications for 181 days
Chronic polypharmacy ≥ 5 medications in 1 month for 6 months
(consecutive or not) in a year
6.
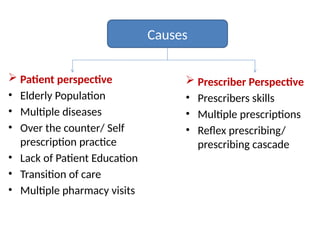
Causes
Patient perspective
•Elderly Population
• Multiple diseases
• Over the counter/ Self
prescription practice
• Lack of Patient Education
• Transition of care
• Multiple pharmacy visits
Prescriber Perspective
• Prescribers skills
• Multiple prescriptions
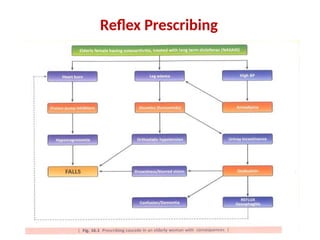
• Reflex prescribing/
prescribing cascade
7.
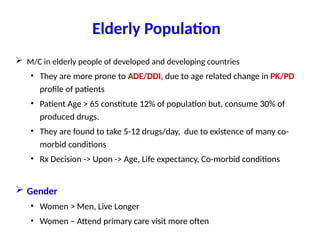
Elderly Population
M/Cin elderly people of developed and developing countries
• They are more prone to ADE/DDI, due to age related change in PK/PD
profile of patients
• Patient Age > 65 constitute 12% of population but, consume 30% of
produced drugs.
• They are found to take 5-12 drugs/day, due to existence of many co-
morbid conditions
• Rx Decision -> Upon -> Age, Life expectancy, Co-morbid conditions
Gender
• Women > Men, Live Longer
• Women – Attend primary care visit more often
8.
Multiple Diseases:Patient suffering from > 1 disease at
a time, which needs multiple medications to treat such
condition.
To reduce his/her long term risk for those condition.
Ex: Diabetes, HTN, Arthritis
Self Medications: Patients takes medicines without
consultation of physician. They are exposed to ADR/DDI.
Neither Health Care person nor Patient consider them
as medicines and take without consultation.
Ex: OTC, Dietary Suppliments
Transition ofcare: Means movement of patient between
different care settings
• Hospitals – Between different levels
• Hospital to Residential Care and vice versa
• In every case of transition – New medicine is added / changed
• Different care providers
Lack of Education:
• Lack of Patient education – Most common - Reason
• Patients don’t ask Questions
• Doctor don’t inform Patients
11.
Prescriber Perspective
• MultiplePrescriptions: Multiple
doctors prescribe medications for
same patient leads to growing list of
medications/drugs to patient.
• Mid level prescribers,
Physicians assistants -
• Not considering the cost vs
benefit
• Not assessing the risk vs benefit
12.
Prescribers Skill
• Dueto improper diagnosis / Lack of knowledge of
potential out comes, he/she might prescribe drugs that are
not necessary/ inappropriate in particular disease
• Symptom based Rx rather than proper diagnosis based Rx
• Physician changes from one medicine to another medicine
of same class.
• Increases exposure to ADR/DDI
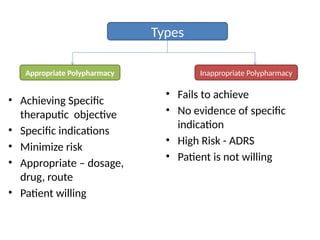
Types
Inappropriate Polypharmacy
Appropriate Polypharmacy
•Achieving Specific
theraputic objective
• Specific indications
• Minimize risk
• Appropriate – dosage,
drug, route
• Patient willing
• Fails to achieve
• No evidence of specific
indication
• High Risk - ADRS
• Patient is not willing
15.
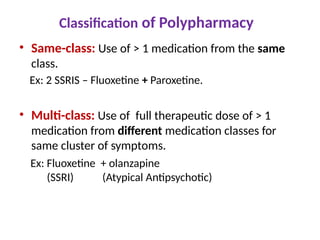
Classification of Polypharmacy
•Same-class: Use of > 1 medication from the same
class.
Ex: 2 SSRIS – Fluoxetine + Paroxetine.
• Multi-class: Use of full therapeutic dose of > 1
medication from different medication classes for
same cluster of symptoms.
Ex: Fluoxetine + olanzapine
(SSRI) (Atypical Antipsychotic)
16.
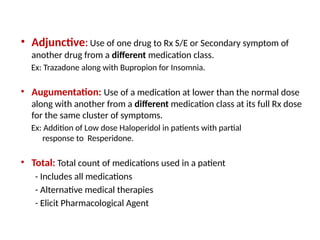
• Adjunctive:Use ofone drug to Rx S/E or Secondary symptom of
another drug from a different medication class.
Ex: Trazadone along with Bupropion for Insomnia.
• Augumentation: Use of a medication at lower than the normal dose
along with another from a different medication class at its full Rx dose
for the same cluster of symptoms.
Ex: Addition of Low dose Haloperidol in patients with partial
response to Resperidone.
• Total: Total count of medications used in a patient
- Includes all medications
- Alternative medical therapies
- Elicit Pharmacological Agent
17.
Consequence/Outcomes
Positive outcomes:
• Synergisticcombination
- Allow lower doses,↓ ADEs than individual drugs
- Ex: Rx HTN
• Supplemental Drugs
- ↓ adverse effect on initial drug
Ex: Anti cholinergic added for drug induced extrapyramidal effects
• Additional Drugs - Improves outcome
Ex: Spironolactone to ACEIS for Heart Failure
• Multiple Drugs - Needed for multiple conditions
Ex: DM + HTN
18.
Negative Outcomes
• DuplicationTherapy: Due to availability of multiple
variety i.e Generic, Brand generic/Brand Name versions
of same medication leads to repetition of same drug.
- Lack of Awareness, Lack of Regular review /
monitoring of drug regimen.
- Often patient visits to multiple prescribers
19.
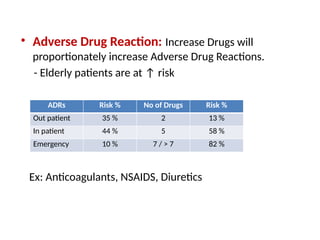
• Adverse DrugReaction: Increase Drugs will
proportionately increase Adverse Drug Reactions.
- Elderly patients are at ↑ risk
Ex: Anticoagulants, NSAIDS, Diuretics
ADRs Risk % No of Drugs Risk %
Out patient 35 % 2 13 %
In patient 44 % 5 58 %
Emergency 10 % 7 / > 7 82 %
20.
• Drug Interactions:
Incidenceof drug interaction increases proportionately
due to increase in number of medicines.
Risk group:
- Elderly Patients
- Multiple co-morbidities
- Lack of nutrition (affect PK/PKD of drug)
21.
• Economic Burden:
-Mismanaged polypharmacy
contributes economic burden
to both the Patient and
Health care system.
22.
• Decreased adherenceand compliance:
- Due to complex drug regimen
- Incomplete explanation of benefits and S/E.
- Lack of communication between patients and
physician
• Impairment quality of life:
- ↓ physical functioning and ↓ ability to carry out
instrumental activities of daily living.
- M/C seen in elderly patients
23.
• Worsening ofDoctor and
Patient relationship:
- Due to ↓ of health status of
patient, he looses belief on
physicians treatment (taking so
many medicine but not feeling
well).
24.
Management
Aim: Should alwaysprohibit
inappropriate polypharmacy.
Reduce overall
polypharmacy
Multiple tools and
techniques which
Detects and reduces
Promotes Evidence based
deprescribing and safe
prescribe
SAIL Techniques
S: Simple
•Regimen should be Simple
• OD/BD is preferred
• Titrated to ideal doses
• FDCs preferred to ↓ pill burden
A: Adverse Effects
• Know about potential ADE of
Medication. identifies the drug using
for treating S/E of the drug
• If possible the drug causing S/E is
discontinued.
28.
I: Indication
Medicationshould have an indication and defined
realistic therapeutic goal.
L: List
Name and Dose of each medication should be written in
the chart and shared with the patient.
29.
TIDE - Technique
T:Time
Appropriate time should be given to
the patient to address and discuss the
medication issues
I: Individualise
Medication should be selected based
on PK and PD principles for individual
patients
Medication or doses should be
individualized based on patient’s
renal/hepatic function
“Start low - Go Slow”
30.
D: Drug- Drug/Drug–Disease
Potential Drug – Drug and Drug-Disease interaction
should be considered/evaluated and avoided.
E: Education
Patients and care givers are educated about
Pharmacological and Non-pharmacological treatments,
ADE,D-D/I, and Monitoring parameters should be
discussed.
31.
Beers Criteria
Beer’scriteria, named after Mark . H. Beers, in 1991, is used
by health care providers & practitioners to improve care in
elderly patients.
Updated in 1997, 2003, 2012, 2019 and 2023.
• Reduces exposure to PIMs-By improving Medication
selection, educating clinicians and patients.
Evaluates quality of care, cost and pattern of dug usage in
older adults.
32.
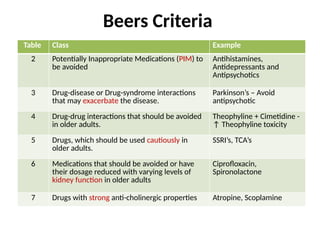
Table Class Example
2Potentially Inappropriate Medications (PIM) to
be avoided
Antihistamines,
Antidepressants and
Antipsychotics
3 Drug-disease or Drug-syndrome interactions
that may exacerbate the disease.
Parkinson’s – Avoid
antipsychotic
4 Drug-drug interactions that should be avoided
in older adults.
Theophyline + Cimetidine -
↑ Theophyline toxicity
5 Drugs, which should be used cautiously in
older adults.
SSRI’s, TCA’s
6 Medications that should be avoided or have
their dosage reduced with varying levels of
kidney function in older adults
Ciprofloxacin,
Spironolactone
7 Drugs with strong anti-cholinergic properties Atropine, Scoplamine
Beers Criteria
33.
START-criteria
• Screening toolto alert
DOCTORS to right treatment.
• Evidence- based prescribing
according to body system to
use at the time of prescribing.
34.
STOPP-Criteria
• Design toidentify
potentially
inappropriate
medications in older
person
• Can be used in
medication review
purpose.
35.
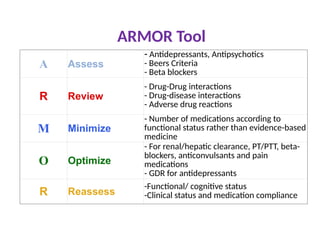
ARMOR Tool
A Assess
-Antidepressants, Antipsychotics
- Beers Criteria
- Beta blockers
R Review
- Drug-Drug interactions
- Drug-disease interactions
- Adverse drug reactions
M Minimize
- Number of medications according to
functional status rather than evidence-based
medicine
O Optimize
- For renal/hepatic clearance, PT/PTT, beta-
blockers, anticonvulsants and pain
medications
- GDR for antidepressants
R Reassess
-Functional/ cognitive status
-Clinical status and medication compliance
37.
Anticholinergic Cognitive Burdenscale
• It is used to assess the cumulative burden of
Anticholinergic drugs.
• Leads to cognitive impairment, confusion, falls and
increased hospitalisation.
• Scoring scale – 4 Categories [ 0 - 3 ]
• 0 - No ACB
• 3 - High
Ex: Alprazolam, Codeine, Atropine
38.
Medication- reconciliation
• Itthe process of comparing a patients medication orders
to all of the medications that the patients has been
taking.
• Done at every transition of care in which new
medications are ordered along with existing medicine.
• Advantage- Avoid medication errors, DDI, Duplications,
Dosing errors.
39.
BROWN - BagTechnique
• Where the patient has to bring all of
his/ her medications in a bag to the
visit.
• Which will be reviewed and if required
then confirm it from different sources.
• This is done by Eliciting Best Possible
Medication History / BPMH.
• Make a list of medications to be
prescribed.
40.
• Compare themedications on the two lists
• Make clinical decisions based on the patient’s condition
(medical, social and financial)i.e. recommend change
with strong justification.
• Communicate the new prescription to the patient/ their
caregivers with proper counseling.
41.
Deprescribing
It isa process of tapering, stopping, discontinuing or
withdrawing drugs with the goal of managing
polypharmacy and improving outputs.
Perform a comprehensive medication reconciliation.
Consider overall risk of drug induced harm.
42.
• Assess eachmedication for eligibility to be
discontinued.
• Prioritize medications for discontinuation.
• Implement drug discontinuation plan and monitor
adverse withdrawal effects.
43.
Role of PPPP
Physician
•Determine all medications being taken.
• Identify the indication for all medications
• When possible select agents with less frequent dose in
schedule.
• Keep drug regimen as simple as possible
• Review all medications profiles routinely.
• Identify any potential adverse effects for each medications
44.
Clinical Pharmacologist
• Cangive their best expertise opinion
• In medical reconciliation
• Prescription repositioning
• Advise on deprescribing
• Proper dose adjustment
• Medical reconciliation OPD services
• Started first at School of Tropical Medicine, Kolkata
– Prof Dr Santanu Kumar Tripathi,
HOD. Dept of Clinical & Experimental Pharmacology
45.
Patient
• The mostimportant thing one can do is to get involved in
his/her own health care.
• Should know the name, strength, S/E, Drug Interactions.
• Follow brown bag technique.
• If one cannot remember whether he/she has taken medicine,
he can try med. dispenser.
• Expiry date should be checked
• Store medicines in a cool dry place.
46.
Pharmacist
• Hospital pharmacist-review the complete and accurate list of
the patient’s medication and evaluate the list of drugs.
• Evaluate problems that arise when medications are
discontinued and initiated during hospitalization.
• Community pharmacist- Play vital role by preventing the
dispensing of unnecessary, inappropriate, side effect prone
medications.
47.
Programmes
Aim :Protect patient from harm arising from polypharmacy by
implementing programmes .
Multidisciplinary Collaboration.
3rd
–WHO- Global patients safety challenge. Medication without harm
Assess successful polypharmacy management activities and advise entire
health system to address management of polypharmacy.
PESTEL - P – Political, E - Economic, S - Social,
T - Technological, E - Environmental, L – Legal.
SWOT - S - Strength, W - Weakness,
O - Opportunities, T - Threats
OPERAM
• Optimizing therapyto prevent avoidable hospital
admission in the multi morbid elderly.
• Aim :To optimize existing pharmacological and non
pharmacological therapies to reduce avoidable hospital
admissions.
• Goal :To access impact of structured medication review
with software intervention
• Finds which is more effective, safe to determine best
and most cost effective measure which prevents
avoidable hospital admissions.
50.
PREMA-eDS
Reduction ofinappropriate medication and adverse drug events in
older populations by electronic decision support.
Aim: To provide physicians with best evidence regarding medication
therapy through an electronic decision support.
Tools:
Indication Check Systematic reviews
Drug interaction Database Renal dosing database
Recommendation based on guidelines Adverse effects database
Disadvantages : Data entry is time consuming
51.
SIMPATHY
• Stimulating InnovationManagement of Polypharmacy
and Adherence in The Elderly.
• Aim: To contribute in developing efficient and sustainable
health care systems
• A set of approaches and tools was developed to help
health service providers to advance current practice by
implementing organizational change.
• Thereby improves polypharmacy.
52.
Recent Advances
Itis important to find innovative solutions to improve
medication, adherence and develops strategies to ensure
Right Medicine Right Time
Artificial Intelligence Large Print Labels
Memory Aids Mobile Applications
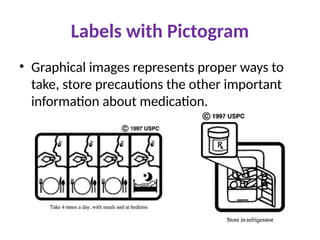
Labels with pictograms Smart Pill Boxes
Reminder Applications
Approaches likely to be increasingly adopted in the future
53.
Artificial Intelligence
Stimulationof human
intelligence in machines that
are programmed to think like
humans and mimic their
actions.
It is easy to detect possible drug
interaction and risk in their
prescription to physicians.
54.
Used to analyzemedical data, patient records, imaging
scans, and genetic information, to assist healthcare
professionals in diagnosing diseases and planning
treatments
Disadvantage: Data Privacy and Ethical challenge need
to be addressed.
55.
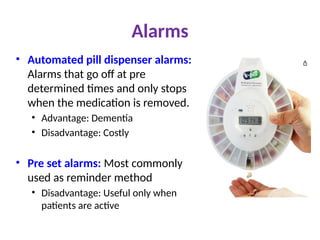
Alarms
• Automated pilldispenser alarms:
Alarms that go off at pre
determined times and only stops
when the medication is removed.
• Advantage: Dementia
• Disadvantage: Costly
• Pre set alarms: Most commonly
used as reminder method
• Disadvantage: Useful only when
patients are active
References
1. POSTGRADUATE PHARMACOLOGYby Sougata Sarkar, Vartika Srivastava, Manjushree Mohanty. 1st
Edition 2020.
2. Postgraduate Topics Pharmacology by Rituparna Maiti 3rd Edition.
3. Medication Safety in Polypharmacy. Geneva: World Health Organization; 2019
(WHO/UHC/SDS/2019.11). Licence: CC BY-NC-SA 3.0 IGO.
4. PATTERN OF MEDICATION USE AMONG ELDERLY PATIENTS ATTENDING MEDICINE DEPARTMENT IN A
TERTIARY CARE HOSPITAL IN INDIA. By SWATHI B, BHAVIKA D. ASIAN OURNAL OF PHARMACEUTICAL
AND CLINICAL RESEARCH, Vol9, Issue 6, 2016
5. American Geriatrics Society 2023 updated AGS Beers Criteria® for potentially inappropriate medication
use in older adults. By the 2023 American Geriatrics Society Beers Criteria® Update Expert Panel.
6. The epidemiology of polypharmacy by Rupert A Payne .
https://www.rcpjournals.org/content/clinmedicine/16/5/465#:~:text=The%20word%20polypharmacy
%20is%20derived,a%20clinical%20definition%20of%20polypharmacy.
7. https://theconversation.com/always-forgetting-to-take-your-medicines-here-are-4-things-that-could-
help-193717
8. https://www.scriptability.com/scriptview-large-print-labels
9. https://www.usp.org/health-quality-safety/usp-pictograms
10. https://www.hmpgloballearningnetwork.com/site/altc/content/armor-a-tool-evaluate-polypharmacy-
elderly-persons



![Anticholinergic Cognitive Burden scale
• It is used to assess the cumulative burden of
Anticholinergic drugs.
• Leads to cognitive impairment, confusion, falls and
increased hospitalisation.
• Scoring scale – 4 Categories [ 0 - 3 ]
• 0 - No ACB
• 3 - High
Ex: Alprazolam, Codeine, Atropine](https://image.slidesharecdn.com/polypharmacy2503-251229094258-3cf13609/85/Polypharmacy_2503-pptx-Polypharmacy_2503-pptx-37-320.jpg)