Polypharmacy and Deprescribing
Polypharmacy= ≥5 medications
…but the real issue is inappropriate polypharmacy.
Prevalence: ↑ from 30% (2005) → 36% (2011)
Common causes: multimorbidity, multiple prescribers, supplements
Risks:
• ADRs, falls, confusion, cost, nonadherence
Distinguish between:
• Appropriate (beneficial, evidence-based)
• Inappropriate (duplicated, no indication, unsafe)
3.
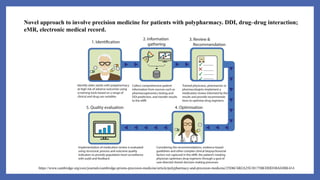
Novel approach toinvolve precision medicine for patients with polypharmacy. DDI, drug–drug interaction;
eMR, electronic medical record.
https://www.cambridge.org/core/journals/cambridge-prisms-precision-medicine/article/polypharmacy-and-precision-medicine/25D6C6B2A25E38175BEDDD3BAE8BE414
4.
Underuse & STARTCriteria
• Underprescribing = Missing beneficial drugs
• Occurs in 20–70% of older adults
• Commonly underused meds:
• Antiplatelets, statins, osteoporosis meds, ACE inhibitors
• Causes:
• Age bias, fear of polypharmacy, lack of geriatric data
• Use START criteria → ensures essential, evidence-based drugs are prescribed
5.
Nonadherence
• Even appropriatetherapy fails without adherence
• Common (6–55% in older adults)
• Causes:
• Cognitive or sensory decline
• Cost, complex regimens, low literacy
• Swallowing or dexterity issues
• Pharmacist actions:
• Simplify schedules
• Use pill boxes, calendars, large labels
• Engage caregivers and check understanding
Ask:
1.How do you take your
meds?
2.How do you remember?
3.How do you afford
them?
4.How often do you miss
doses?
6.
Comprehensive Geriatric Assessment
(CGA)
•Holistic review to optimize pharmacotherapy
• Steps:
Collect a complete medication and supplement history
Match each drug to its indication
Identify PIMs and omissions (Beers / STOPP / START)
Assess adherence, interactions, and duplicate therapy
Set age-appropriate goals (symptom control > prevention in frailty)
7.
Deprescribing (Applied)
• Systematicwithdrawal of unnecessary medications
• Done when:
• Risks > benefits
• Misaligned with patient’s goals or life expectancy
• Steps:
• Identify candidate meds (use Beers, STOPP)
• Discuss with patient/caregiver
• Taper or stop gradually (avoid withdrawal reactions)
• Document and monitor outcomes
• Be alert for Adverse Drug Withdrawal Events (ADWEs) — e.g., rebound HTN,
insomnia
8.
Pharmacist’s Role
• Pharmacists= Medication Safety Advocates
• Identify, prevent, and report ADRs
• Conduct medication reconciliation at care transitions
• Provide MTM (Medication Therapy Management) and deprescribing plans
• Educate patients, families, and healthcare teams
• Use tools & evidence to personalize therapy
9.
Targeting High-Risk Patients
•Prioritize medication review for:
• ≥5 chronic meds
• Using anticoagulants, opioids, insulin, NSAIDs, antipsychotics
• Frailty, cognitive decline, frequent hospitalizations
• Recent medication changes or multiple prescribers
• Goal: Focus resources on those most likely to benefit from intervention
10.
Tools and Criteriafor Safe Geriatric
Prescribing
•Beers Criteria (American Geriatrics Society)
•STOPP/START Criteria (Screening Tool of Older Persons’ Prescriptions)
•Medication Appropriateness Index (MAI)
•FRIDs (Fall-Risk-Increasing Drugs) lists
Communication and Counseling
Assess health literacy and hearing/vision limitations
Simplify medication regimens and labeling
Encourage use of pill organizers, medication charts
Involve caregivers in counseling
13.
Adverse Drug ReactionPrevention
• 7 Key Prevention Strategies:
• Assess comorbidities, cognition, frailty
• Adjust doses for renal/hepatic function
• Limit number of meds
• Monitor drug effects/labs
• Watch for atypical symptoms (e.g., confusion = UTI or ADR)
• Match therapy to life expectancy
• Identify self-medication & OTC use
14.
Undertreatment (Underprescribing)
• Commonomissions:
• Anticoagulants for Afib (bleeding fear)
• β-blockers in HF
• Statins for ASCVD
• Analgesics for pain
• Antihypertensives for stroke prevention
15.
• Textbooks
1.Pharmacotherapy: APathophysiologic Approach by DiPiro et al. (12th Ed.)
• Chapter: e23 “Geriatrics: Physiology of Aging”
2.Geriatric Dosage Handbook by Lexicomp
3.Goodman & Gilman’s The Pharmacological Basis of Therapeutics (14th Ed.)
#2 Polypharmacy
Definition: Use of ≥5 medications or any unnecessary/duplicated therapy.
Common in older adults due to multiple chronic diseases.
Consequences:
↑ Risk of adverse drug reactions (ADRs)
↑ Drug–drug and drug–disease interactions
↓ Adherence and ↑ medication costs
Functional decline, confusion, falls, and hospitalizations
Principles of Safe Medication Review
Review all current medications and their indications.
Identify high-risk drugs (anticholinergics, benzodiazepines, NSAIDs, hypoglycemics).
Assess ongoing need and benefit versus harm.
Check for duplication, interactions, and alignment with patient goals.
Deprescribing Process (Mini-Algorithm)
List all meds + indication.
Identify PIMs / duplicates / interactions.
Align with patient goals (function, comfort, safety).
Trial taper/stop highest-risk, lowest-benefit drug first.
Monitor & document outcomes; involve patient & caregiver.
Beers Criteria → avoid high-risk drugs
STOPP → identify meds to stop
START → identify meds to start
Clinical Example:
Case:
79-year-old female with HTN, DM, insomnia, arthritis.
Meds: Amlodipine, Metformin, Glyburide, Diclofenac, Diazepam, Diphenhydramine.
Actions:
Stop diphenhydramine (anticholinergic, fall risk).
Taper diazepam (sedation, dependence).
Switch glyburide → glipizide (lower hypoglycemia risk).
Review diclofenac use; consider safer pain alternatives.
Key Takeaways
“Start low, go slow, but go!” — don’t stop everything at once.
Reassess renal, hepatic, and cognitive status regularly.
Engage patients and caregivers in shared decision-making.
Document rationale and follow-up every 2–4 weeks.
#6 Beers, STOPP/START, MAI (Medication Appropriateness Index)
#11 Example:
79-year-old female, HTN, diabetes, insomnia, arthritis.
Meds: amlodipine, metformin, glyburide, diclofenac, diazepam, diphenhydramine (OTC sleep aid).
Patient:
79-year-old female
Chronic conditions: hypertension, diabetes, insomnia, arthritis
Current Medications:
Amlodipine
Metformin
Glyburide
Diclofenac
Diazepam
Diphenhydramine (OTC sleep aid)
Step 1 – List all meds + indications
Amlodipine → Hypertension
Metformin → Type 2 Diabetes
Glyburide → Type 2 Diabetes
Diclofenac → Arthritis pain
Diazepam → Insomnia
Diphenhydramine → Sleep aid
Step 2 – Identify PIMs / duplicates / interactions
Glyburide: high risk of hypoglycemia in elderly
Diazepam + Diphenhydramine: additive CNS depression → confusion, falls
Diclofenac: GI bleed and renal risk in long-term use
Step 3 – Align with goals
Maintain BP and glucose control
Improve sleep without sedation or falls
Reduce pain safely
Minimize pill burden and adverse events
Step 4 – Trial taper / stop (highest-risk, lowest-benefit first)
Taper diazepam over 2–4 weeks → replace with sleep hygiene or melatonin
Stop diphenhydramine → anticholinergic burden
Switch glyburide → glipizide (shorter acting, safer)
Review need for diclofenac → consider acetaminophen or topical NSAID
Step 5 – Monitor & document outcomes
Reassess glucose, pain, and sleep in 2–4 weeks
Ask about alertness, falls, mood, and adherence
Update medication list and communicate with caregiver
#12 se Tools to Guide Deprescribing:
Beers Criteria → avoid high-risk drugs
STOPP → identify meds to stop
START → identify meds to start
MAI → assess appropriateness
Anticholinergic burden scales → assess cognitive risk
#17 1 — SMART Aim & Measurement
SMART Aim:
Reduce high-risk ADRs in adults ≥65 by 25% in 12 weeks on Ward/Clinic ___.
Population: ≥65 years OR ≥5 meds OR using high-risk drugs (anticoagulants, hypoglycemics, opioids, anticholinergics, FRIDs).
Measures
Outcome: ADRs/100 patient-days; falls w/ injury; hypoglycemia <70 mg/dL; AKI (KDIGO); 30-day med-related ED visits/readmits.
Process:
Med rec completed ≤24 h (yes/no)
Renal dose verified (CG CrCl used & weight choice documented)
Beers/STOPP flag recorded
Anticholinergic burden score (e.g., ACB) documented
% discharges with indication + stop date on each med
Balancing: sleep disturbance score, uncontrolled pain, length of stay, time burden.
Team: Pharmacist (lead), MD/NP, RN, QI, IT/EMR, PT/OT (falls), Case Mgmt.
2 — PDSA 1: Admission Med Rec + Beers Screen
Plan
Pharmacy-led Best Possible Medication History within 24 h.
1-page checklist: indication match, duplicate therapy, Beers/STOPP flags, ACB score.
Do
Pilot on 1 unit for 2 weeks; weekday hours only.
Study
% med rec ≤24 h
PIMs identified/patient; # actions (hold/stop/change)
Early ADR signals (confusion, orthostasis)
Act
Spread to weekends; add quick order phrases “Avoid per Beers (reason)”.
3 — PDSA 2: Renal Dosing Safety-Stop
Plan
Cockcroft–Gault auto-calc (actual/ideal/adjusted weight rule embedded).
Hard-stop pharmacist verification for renally cleared meds (e.g., DOACs, gabapentin, TMP-SMX, digoxin).
Do
Turn on alert for ≥65 years or SCr change ≥0.3 mg/dL/48 h.
Study
% appropriate renal dosing at first order
AKI-linked ADRs/100 pt-days
Alert acceptance rate & override reasons
Act
Tweak thresholds; add creatinine trend banner; target high-override prescribers with tip sheet.
4 — PDSA 3: FRIDs → Safer Sleep & Fall Bundle
Plan
STEADI screen; deprescribe benzos/Z-drugs/diphenhydramine where feasible.
Non-drug sleep bundle (lights/noise, mobilize, pain plan, melatonin PRN).
Do
Night shift nurse checklist + pharmacist bedtime MAR sweep.
Study
Sedative DDD/100 pt-days; ACB score change; falls/1000 pt-days.
Act
Standardize zolpidem stop + CBT-I handout on discharge; add PT balance class referral.
5 — PDSA 4: Safer Discharge & 72-h Call
Plan
Discharge med list must include indication & stop date for antibiotics, steroids, PPIs, sleep meds.
Teach-back + printed “When to call us” card.
Do
Pharmacist phones patient/caregiver at 72 h to reconcile fills, side effects, adherence barriers.
Study
% discharges with complete med list; post-discharge med issues found/corrected; 30-day med-related ED/Readmit.
Act
Auto-populate indications from problems list; enroll high-risk pts into follow-up calls.
6 — Tools & Checklists (What to Use)
Beers (AGS), STOPP/START, MAI, ACB scale
CrCl calculator with weight logic:
Normal BMI → actual or ideal (per policy)
Underweight → actual
Obese → adjusted (IBW + 0.4×[ABW–IBW])
Med Rec form: Drug–Indication–Risk–Action–Monitoring
Deprescribing algorithms (benzos, PPIs, anticholinergics)
STEADI screen card; Teach-Back script
7 — Data & Visuals (how to track quickly)
Daily tally sheets → weekly run charts for:
ADRs/100 pt-days
Renal-dose-verified rate
ACB average per patient
Falls/1000 pt-days
Annotate chart with P, D, S, A dates to see impact.
8 — Common Barriers → Fast Fixes
Alert fatigue: limit to high-harm meds; require reasoned overrides.
Time pressure: technician-assisted med rec; use home pharmacy fill history.
Clinician buy-in: share 1-minute case of avoided harm each huddle.
Patient factors: low literacy → pictogram med list; cost → $4 list/manufacturer assistance.
9 — Mini PDSA Card (print for huddles)
PLAN: Aim, who/where, 2 measures, prediction
DO: Dates, what changed, issues
STUDY: Data vs prediction, brief learning
ACT: Adopt / Adapt / Abandon; next test
10 — Example Results Statement (to model)
“After 6 weeks, renal-dose verification rose from 62% → 91%; AKI-linked ADRs fell 38%; balancing: no increase in undertreatment (stable pain/sleep scores). We’ll adopt the alert and adapt weight logic for extreme BMI.”
#18 Koda-Kimble and Young’s Applied Therapeutics: The Clinical Use of Drugs
Clinical Guidelines & Databases
American Geriatrics Society (AGS) Beers Criteria® (2023 Update)
https://geriatricscareonline.org
STOPP/START Criteria (2nd or 3rd Edition) https://pubmed.ncbi.nlm.nih.gov/
Lexicomp / Micromedex / UpToDate — for drug dosing and interactions
NCBI Bookshelf / PubMed — for open-access reviews and case studies
National Institute on Aging (NIA) — https://www.nia.nih.gov/
World Health Organization (WHO) – Medication Safety in the Elderly
Journals and Articles
Drugs & Aging (Springer)
Journal of the American Geriatrics Society (JAGS)
Age and Ageing (Oxford Academic)
Annals of Pharmacotherapy






























![deprescribing [Autosaved].pptx deprescribing](https://cdn.slidesharecdn.com/ss_thumbnails/deprescribingautosaved-241223133144-3e056194-thumbnail.jpg?width=640&height=640&fit=bounds)






















