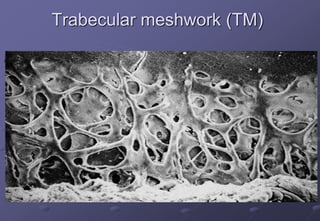
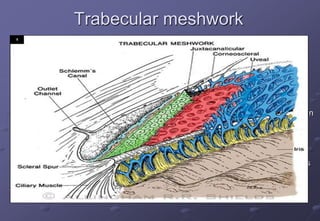
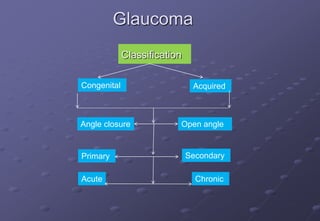
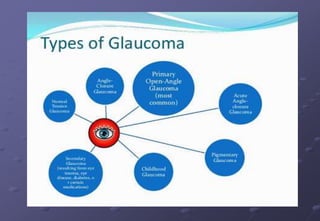
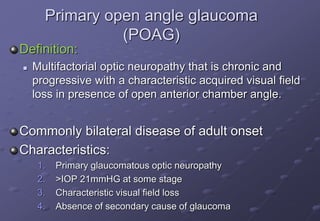
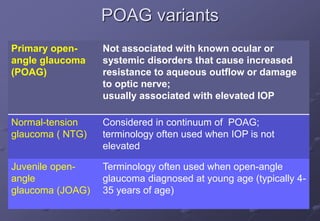
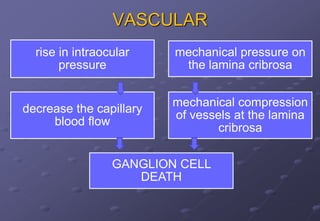
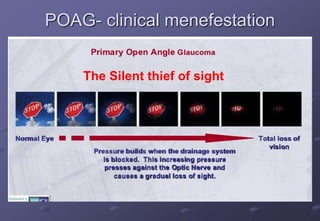
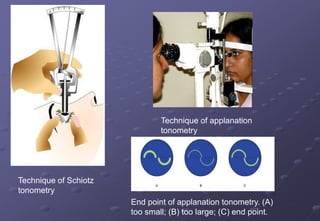
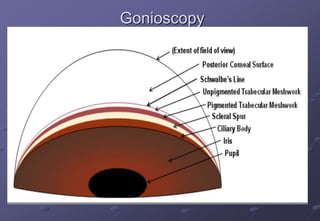
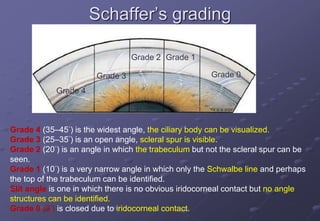
This document provides an overview of primary open-angle glaucoma (POAG). It discusses the pathophysiology of raised intraocular pressure in POAG, risk factors, genetics, clinical presentation, investigations including tonometry and gonioscopy, and management principles. POAG is the most common type of glaucoma and results from obstruction of aqueous outflow, leading to optic nerve damage and visual field loss. Family history, older age, higher IOP levels, and conditions like myopia and diabetes increase risk. Genetic factors and changes in the trabecular meshwork contribute to outflow obstruction in POAG.

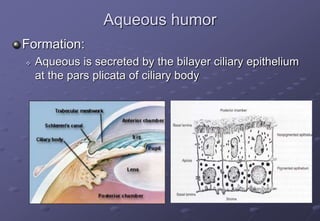




























![AQEOUS_HUMOUR_PHYSIOLOGY_AND_GLAUCOMA3_(1)[1].pptx](https://cdn.slidesharecdn.com/ss_thumbnails/aqeoushumourphysiologyandglaucoma311-250407162804-3ddea82a-thumbnail.jpg?width=640&height=640&fit=bounds)






























