Approach
• Basic physiology/anatomyof the adrenal gland
• Definition of Addison’s disease
• Causes and presentation
• Diagnosis
• Management and patient follow up.
3.
Introduction
• The adrenalglands each weighs about 4g and located
at the upper poles of each kidney
• They have 2 distinct zones- cortex which secretes the
mineralocorticoid, glucocorticoid and androgen
hormones.
• The medulla secretes epinephrine and norepinephrine.
• Secretion of the cortex hormones is under the
influence of the hypothalamus-pituitary-adrenal axis
and the RAAS system.
4.
Introduction cont
• Whereas for the medulla hormones s under the
sympathetic neurohormonal stimulation.
• The gland is important in:
• Metabolism and immune response through
glucocorticoids
• Blood pressure and vascular volume and electrolyte
control through the mineralocorticoids.
• Secondary sexual characteristics in females through
androgens.
5.
cont
• Adrenal glanddisorders may be due to
hyperfunction ( Cushing’s syndrome) or hypofunction
(adrenal insufficiency) or genetic abnormalities of
steroid genesis
• Characterized by reduced glucocorticoid hormone
secretion.
• Daily corticoid secretion ranges from 15-30mg/m2
with a circadian cycle.
• Levels are determined by the rate of secretion, rate
of inactivation and excretion of free cortisol.
• Inactivation of steroids primarily takes place in the
liver
6.
Addison’s disease
• Note:adrenal insufficiency can arise either because of
inadequate ACTH function/release or failure of the
adrenal gland to secrete sufficient levels of hormones.
• Addison’s disease is a primary failure of the adrenal
gland to elaborate adequate levels of glucocorticoids.
• It results from progressive destruction of the adrenal
gland of greater than 90% for the insufficiency to
appear.
7.
Causes of Addison’sdisease
Anatomic destruction of the gland-acute or chronic.
-Autoimmune, surgical removal, haemorhage, metastatic invasion
Infections- Viral-HIV, CMV,EBV, Fungal, bacterial eg TB.
Metabolic failure in hormone production eg Congenital adrenal hyperplasia,
enzyme inhibitors( ketoconazole, metyrapone,phenytion, Rifampicin
Rare: ACTH blocking antibodies, Mutation, Infiltrative conditions
Patients with autoimmune adrenal failure can have other failure like-
Thyroiditis, Type 1 DM, Hypo or hyperthyroidim, premature ovarian failure
etc. panicious anemia, vitiligo ,alopecia, mysthenia gravis.
Presentation of Adrenalfailure
•
• Symptoms are insidious in onset.
• Non specific- fatigability, weakness, anorexia, nausea,
vomiting, wgt loss, cutaneous and mucosa
pigmentation, hypotension and some times
hypoglycaemia
• Symptoms depend on severity, duration and vary
from chronic mild fatique to severe shock.
10.
Cont
• GIT symptomsmay be the presenting symptoms in
some cases: Anorexia, wgt loss, nausea, vomiting,
diarrhea, non specific abdominal pain.
• May have mood changes with excessive irritability,
restlessness.
• May have scanty axillary and pubic hair in females
due to loss of adrenal androgen
11.
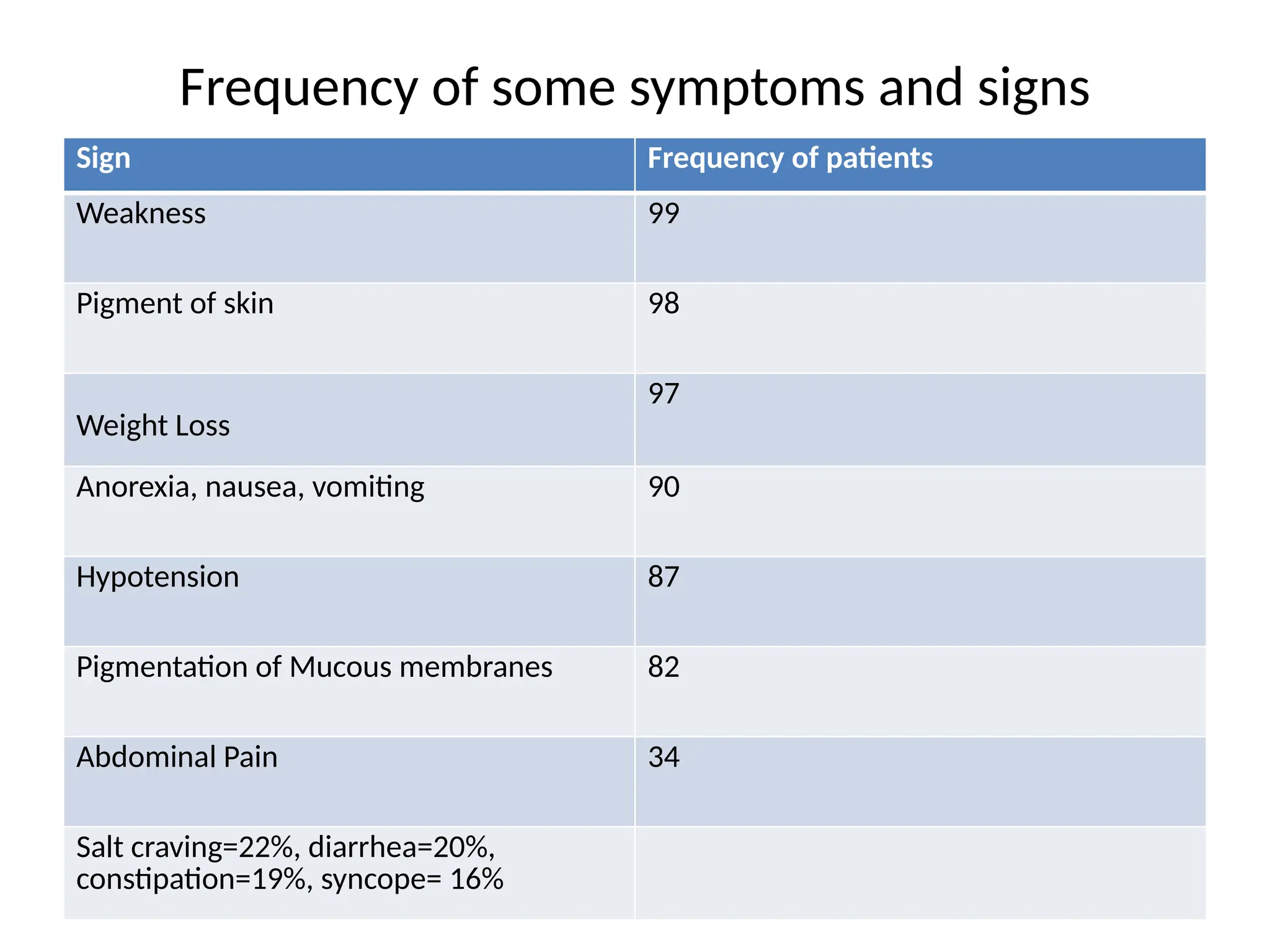
Frequency of somesymptoms and signs
Sign Frequency of patients
Weakness 99
Pigment of skin 98
Weight Loss
97
Anorexia, nausea, vomiting 90
Hypotension 87
Pigmentation of Mucous membranes 82
Abdominal Pain 34
Salt craving=22%, diarrhea=20%,
constipation=19%, syncope= 16%
12.
Investigations for Addison’sdisease
• Non specific: Plasma electrolytes,
• Low Sodium, chloride, HCO3, elevated potassium.
• Morning plasma cortisol levels, aldosterone levels
• Specific test:
• 1. ACTH stimulation test. This assesses the ability of the
adrenals to produce steroids.
• Give 250ug of cosyntropin IM/IV and measure cortisol levels
after 60 mins. Cortisol leves below 495nmol/L are diagnostic
of adrenal insufficiency.
• To determine if the cause is primary or secondary, measure
ACTH or B-LPT peptides. They are raised in primary failure and
low in secondary.
13.
Making a diagnosis
•
•None of the common symptoms of adrenal failure is
specific.
• They often present in many other diseases.
• Diagnosis therefore requires a high level of suspicion.
• Note the symptom score and what may be consistent
14.
Treatment of Addison’sdisease
• Provide specific hormone replacement.
• It may be glucocorticoid, minerolocortocids or both.
• Cortisol is the main glucococrticoid used.
• Starting dose depends on the size of the patient ( 1-
2mg/kg).
• 2/3 of the dose should be given in the morning and
1/3 in the evening.
• Watch for the S/Es of steriods- irritability, insomnia,
excitement, gastritis and long term complications.
15.
Treatment cont,
• Titrateto the lowest effective dose possible.
• Where there is mineralocorticoid deficiency,
• Use 0.05-1mg of fludrocortisone per day orally. Advise
patients to have good Sodium intake about 3-4 g/day
• Monitor blood pressure and electrolytes.
• Patients with adrenal insufficiency should carry an
identification note on them.
16.
Special considerations
• Duringperiods of acute febrile illness, the dose
of cortisol may need to be increased.
• Before surgery, provide supplemental
glucocorticoid.
• Management does not change in pregnancy
but the drug requirement may increase.









































![ANTIPROTOZAL_DRUGS, overview of different protozoal infections[1].pptx](https://cdn.slidesharecdn.com/ss_thumbnails/antiprotozaldrugs-11-250313192836-f3e3bdb1-thumbnail.jpg?width=640&height=640&fit=bounds)






























![Apporach to lung biopsy [Auto-saved].pptx latest](https://cdn.slidesharecdn.com/ss_thumbnails/apporachtolungbiopsyauto-saved-251211225655-93258539-thumbnail.jpg?width=640&height=640&fit=bounds)




