Personalizing wellness processes to employees will boost engagement, camaraderie, the corporate culture, productivity....and of course health.
We add a new definition of personalized to employee wellness. Course development for private licensing? We still will perform our unique HRA & CCA to develop your perfect e-learning courses.
Live Interactive webinars, Incentive programs with wearable technology......adding your employees own biometrics to the wellness process?? Coming very soon - GENOMICS!
Financial wellness, FARMacy....nutrition, physical activity, minimizing the root of all chronic disease - oxidative stress, stress reduction, family lifestyle, sexual health, sleep.....our coaches are highly specialized experts - who become your employees coaches......personalizing at bulk prices...
FUN, engaging .....creating your corporate health culture
Upping the "Total" in Total Rewards. Incentivizing your employees with the most sophisticated wearable technology, measuring more biomarkers than any other device, and the only device meriting being reviewed as a medical device. Included in the cost of the device - customized wellness programs designed on your employees biometrics. Our commitment to provide the most personalized corporate wellness programs, at the most affordable price and everyone gets the ultimate wearable technology. We will happily help you design a true program of reward - employee/employer contribution - rewarding commitment and motivation.
Workplace Wellness in Flux – Nicolaas Pronk at Modern Healthcare's 8th annual Workplace of the Future Conference on Wednesday, October 14, 2015 at the Omni Hotel in Nashville Tennessee.
Data drives company outcomes - employers agree analytics are a key factor in strategic planning. Customizing wellness solutions that has turned science fiction into science. Employees biometrics and genomics - sequencing the genome - drives choosing individualized wellness coaching. Health solutions - providing a path of sustainability and adherence - scientific, engaging, redefining individualized - And we make it affordable. Employee health programs - what a wonderful way to build healthier communities - establish lifestyle habits creating a healthier future for our children. We can manage & prevent chronic illnesses - saving lives and money - investing the money for happier, bigger, better futures.
Personalizing wellness processes to employees will boost engagement, camaraderie, the corporate culture, productivity....and of course health.
We add a new definition of personalized to employee wellness. Course development for private licensing? We still will perform our unique HRA & CCA to develop your perfect e-learning courses.
Live Interactive webinars, Incentive programs with wearable technology......adding your employees own biometrics to the wellness process?? Coming very soon - GENOMICS!
Financial wellness, FARMacy....nutrition, physical activity, minimizing the root of all chronic disease - oxidative stress, stress reduction, family lifestyle, sexual health, sleep.....our coaches are highly specialized experts - who become your employees coaches......personalizing at bulk prices...
FUN, engaging .....creating your corporate health culture
Upping the "Total" in Total Rewards. Incentivizing your employees with the most sophisticated wearable technology, measuring more biomarkers than any other device, and the only device meriting being reviewed as a medical device. Included in the cost of the device - customized wellness programs designed on your employees biometrics. Our commitment to provide the most personalized corporate wellness programs, at the most affordable price and everyone gets the ultimate wearable technology. We will happily help you design a true program of reward - employee/employer contribution - rewarding commitment and motivation.
Workplace Wellness in Flux – Nicolaas Pronk at Modern Healthcare's 8th annual Workplace of the Future Conference on Wednesday, October 14, 2015 at the Omni Hotel in Nashville Tennessee.
Data drives company outcomes - employers agree analytics are a key factor in strategic planning. Customizing wellness solutions that has turned science fiction into science. Employees biometrics and genomics - sequencing the genome - drives choosing individualized wellness coaching. Health solutions - providing a path of sustainability and adherence - scientific, engaging, redefining individualized - And we make it affordable. Employee health programs - what a wonderful way to build healthier communities - establish lifestyle habits creating a healthier future for our children. We can manage & prevent chronic illnesses - saving lives and money - investing the money for happier, bigger, better futures.
The Leadership Pipeline: Cultivating Your Organization’s High Potential Emplo...Modern Healthcare
The Leadership Pipeline: Cultivating Your Organization’s High Potential Employees – Joseph Cabral at Modern Healthcare's 8th annual Workplace of the Future Conference on Wednesday, October 14, 2015 at the Omni Hotel in Nashville Tennessee.
Why is physician engagement strategically important? How can you design a strategy that is laser-focused on increasing clinical demand by ensuring your medical staff is aligned?
This presentation highlights key data, a framework for focusing your efforts with an aim statement and developing a programmatic approach to physician engagement.
Health, well-being and productivity improvement in the workplaceLimeade
Slides from a webinar with Dr. Michael Parkinson and Limeade.
We spend $2.8 trillion on healthcare but much is attributed to waste or behaviors we can change. The best place for behavior change? The workplace.
The slides review:
- common drivers of health and productivity in the workplace
- how you can address them in your own organization
- 6-step roadmap to improvement
St. Luke's Health System President and CEO Dr. David Pate's presentation to at the state of Idaho's Medicaid Managed Care Public Forum held in Boise on Dec. 13, 2011.
We specialize in the successful placement of all physician specialties and sub-specialties in small rural facilities, large medical centers, healthcare systems, and academics. We ensure that your new physician will integrate well into your community as both a true leader and a valuable asset for your facility.
Healthcare Globally needs a major disruption and a transformative approach to make life sustainable on this planet with the ever increasing threat to Quality of Life.
Uni Papua FC Bali perkenalkan Football 3
Di lapangan Renon Denpasar BALI.
Bersama GM Uni Papua FC
#UniPapuaFootball #UniPapuaFc #Papua #Indonesia
#SepakbolaSosial #Sepakbola #FIFA #UniPapua
#coachesacrosscontinents #oneworldplayproject
#SocialFootball #bali #Soccer #denpasar #renon
#Olahraga #Football #Football3
www.unipapua.net
www.unipapua.net/bali
info@unipapua.net
-Ys-
The Leadership Pipeline: Cultivating Your Organization’s High Potential Emplo...Modern Healthcare
The Leadership Pipeline: Cultivating Your Organization’s High Potential Employees – Joseph Cabral at Modern Healthcare's 8th annual Workplace of the Future Conference on Wednesday, October 14, 2015 at the Omni Hotel in Nashville Tennessee.
Why is physician engagement strategically important? How can you design a strategy that is laser-focused on increasing clinical demand by ensuring your medical staff is aligned?
This presentation highlights key data, a framework for focusing your efforts with an aim statement and developing a programmatic approach to physician engagement.
Health, well-being and productivity improvement in the workplaceLimeade
Slides from a webinar with Dr. Michael Parkinson and Limeade.
We spend $2.8 trillion on healthcare but much is attributed to waste or behaviors we can change. The best place for behavior change? The workplace.
The slides review:
- common drivers of health and productivity in the workplace
- how you can address them in your own organization
- 6-step roadmap to improvement
St. Luke's Health System President and CEO Dr. David Pate's presentation to at the state of Idaho's Medicaid Managed Care Public Forum held in Boise on Dec. 13, 2011.
We specialize in the successful placement of all physician specialties and sub-specialties in small rural facilities, large medical centers, healthcare systems, and academics. We ensure that your new physician will integrate well into your community as both a true leader and a valuable asset for your facility.
Healthcare Globally needs a major disruption and a transformative approach to make life sustainable on this planet with the ever increasing threat to Quality of Life.
Uni Papua FC Bali perkenalkan Football 3
Di lapangan Renon Denpasar BALI.
Bersama GM Uni Papua FC
#UniPapuaFootball #UniPapuaFc #Papua #Indonesia
#SepakbolaSosial #Sepakbola #FIFA #UniPapua
#coachesacrosscontinents #oneworldplayproject
#SocialFootball #bali #Soccer #denpasar #renon
#Olahraga #Football #Football3
www.unipapua.net
www.unipapua.net/bali
info@unipapua.net
-Ys-
An Obstetrics and gynecology presentation: A 20 years old single female undergraduate presents to the emergency unit with fever, lower abdominal pain and abnormal vaginal discharge of 5 days duration. Discuss her management
Dr. Edward Wagner, Director (Emeritus) MacColl Center, Senior Investigator, Group Health Research Institute addresses the 2014 Weitzman Symposium on The Future of Primary Care
HealthcareSource® Behavioral Assessments: Recruit for Higher Retention in Hea...HealthcareSource
By harnessing behavioral assessment solutions from HealthcareSource that are designed to increase retention and improve patient satisfaction, HR teams can help leaders, managers, and employees reduce costs and improve the patient experience—the ultimate goal for any healthcare organization. In addition, Southwest General Health Center shares their success story with using Staff Assessment to develop high performers.
Findings on health information technology and electronic health recordsDeloitte United States
The Deloitte Center for Health Solutions 2016 Survey of US Physicians set out to understand physician adoption and perception of key market trends around health information technology and electronic health record data. Explore key survey findings to discover where physicians find the most value, barriers to adoption, and what they want next. http://deloi.tt/2d3b4w6
Five Data-driven Patient Empowerment StrategiesHealth Catalyst
Data plays a big role toward empowering patients to become more involved in their care. With data, digital tools, and education, patient empowerment can act like a blockbuster drug to produce exceptional outcomes.
Data empowers patients five ways:
Promotes patient engagement.
Produces patient-centered outcomes.
Helps patients practice self-care.
Improves communication with clinicians.
Leads to faster healing and independence.
Clinicians using creative, innovative care strategies, and patients with access to the right tools and technology, can produce remarkable results in terms of cost, health outcomes, and experience.
doctors and nurses can be differentiated in an effortless manner. Doctors study and cure disease, while nurses study and heal people. Too know more visit: https://at.tumblr.com/medicalsaffairsusa/what-can-nurses-do-that-doctors-cannot/31c42h37gaen
The Nurse Leader as Knowledge WorkerHenry Ehizokhale.docxarnoldmeredith47041
The Nurse Leader as Knowledge Worker
Henry Ehizokhale
Walden University
Transforming Nursing And Health Through Technology
NURS 6051
Nov 27, 2019
1
The Nurse Leader as Knowledge Worker
2
Purpose
Explain the concept of a knowledge worker.
Define and explain nursing informatics and highlight the role of a nurse leader as a knowledge worker.
The concept of a knowledge worker
The term “knowledge worker” was first coined by Peter Drucker. Ducker defined knowledge workers as high-level workers who apply theoretical and analytical knowledge, acquired through formal training, to develop products and services (CFI, 2019). He emphasized that due to the high level of productivity and creativity of knowledge worker, that they would be the most valuable assets in the 21st century organization. Professionals that can be referred to as knowledge worker includes engineers, pharmacists, architects, financial analysts, public accountants, physicians, scientists, design thinkers, and lawyers. Furthermore, knowledge workers have a high degree of expertise, experience, education and the primary purpose of their jobs involve the distribution, creation and application of knowledge.
3
Definition of a knowledge worker by Peter Drucker
Professional that are referred to as knowledge worker
Nursing Informatics
Nursing Informatics is a subset of informatics, specific to the nursing field and the role of the nurse in the healthcare setting. There has been several interpretation of nursing informatics. The American Nurses Association (ANA), identified nursing informatics as a specialty that integrates nursing, science, computer science, and information science to manage and communicate data, information, and knowledge in nursing practice (ANA, 2001, pg.17).
4
Nurse leader as a knowledge worker.
A nurse leader is one who inspire others to work together to achieve a common goal, for instance enhanced patient care or satisfaction. All nurses are called to nurse leadership, however there are different levels of nurse leadership. Nurse leaders are expected to help the organization to fulfill the organization’s mission, vision, values, and strategies to achieve long-range plans. Nurse leaders part take in policy setting, overseeing quality measures are carried out, accountability for overall quality of patient care delivery, staff satisfaction and organizational outcomes. For a nurse leader as a knowledge worker to be productive in an organization, the nurse leader must understand that knowledge work requires continuous learning on the part of the knowledge worker, but equally continuous teaching on the part of the knowledge worker. Having said that, a knowledge worker nurse leader will depend hugely on evidenced based practice to be productive in a healthcare organization. The use of EBP by knowledge worker nurse leader will require learning and teaching. Most healthcare organizations or hospitals rely on evidenced based.
The high turnover rate of staff is causing hospital leadership to panic. Given that the cost of replacing a nurse can be upwards of 1.3 times their salaries, hospitals need to understand the reasons why this is occurring. The implications are far-reaching for hospitals and they need to understand how to evolve traditional approaches to stay ahead of the evolving needs of their staff. By taking a proactive approach to talent management, health systems can better hire, retain, and engage today’s workforce.
This presentation by Rebecca Parker, MD, FACEP and Chair of the ACEP Board and Steve Dobberowsky, Principal Consultant of Thought Leadership & Advisory Services at Cornerstone OnDemand, shares strategies to help identify and reduce the risk of staff departures to healthcare organizations.
Steve provides easy-to-understand insights on:
* The biggest challenges health systems have in staff retention (and engagement!)
* Why your team may already be applying to other hospitals
* Talent management strategies that create a more productive, passionate workforce
Medicare and Medicaid In-Patient service' s provided within Nursing Homes for the Mental disabled. These service;s are avaliable through out the United States in every State.Contact us for more information?
Running head SKILLS ASSESSMENT PAPER1SKILLS ASSESSMENT PAPE.docxtodd521
Running head: SKILLS ASSESSMENT PAPER
1
SKILLS ASSESSMENT PAPER
4
Skills Assessment Paper
Summary of Skills
For the development of an organization to be successful and effectively achieve set goals and objectives, strong management and organization skills will be required (Bateman & Snell, 2007). Our Team A brings a broad spectrum of skills and talents coming from life, educational and work-related experiences. Each member of the team possesses unique skill sets that will bring fresh ideas, techniques and creative solutions to challenges in the development of our consulting firm.
A thorough evaluation of our team member’s skills, suggests that our key strengths lie within teamwork and dedication, creating presentations, critical thinking, problem-solving techniques, communication, research, and observations. With these skills, this team will be able to successfully achieve most tasks necessary in the development of a consulting firm. This team will need to use these skills to collaborate efforts in a cooperative manner to create, plan, develop and accomplish the goals of the consulting firm. This evaluation also portrays a strong dedication to learning and improving which is beneficial in the development of new skills that may be needed.
Most members of our team currently have educational and professional experience that proves an intense desire to improve and advocate change and educate communities to collaborate an effort enhancing the lives of individuals. This desire will effectively promote positive changes both within communities as well as at a societal level. The team’s overall commitment is to meet basic human needs through education, focusing on identification of challenges and prevention, as well as assist in overcoming personal and organizational obstacles that individuals may face. Our team is committed to improving the overall quality of life through advocacy and action.
The first type of consulting firm that we could possibly work with would be a human services/independent living consulting program. This program would collaborate with a client’s care givers, doctors and independent care organizations to assist in facilitating a client’s independence and improve or maintain health. This consulting firm would collaborate efforts to create an independent, long-term care plan that will enhance the develop of daily living skills, educate on services and programs available, exercise the right to make healthy living choices, and encourage pro-active involvement of all care-giving professionals in the pursuit of personal growth, presence, and participation in the long term care process. This program will improve and emphasis respect and dignity through the promotion of independence.
PLEASE ADD THE OTHER TWO TYPES HERE!
The types of problems these consulting firms might solve.
Inflexible regulatory and legal issues create competitive obstacles human services providers face when offering health services to communities.
Chocking the Barriers to Change in Healthcare System.By.Dr.Mahboob ali khan Phd Healthcare consultant
Change is undeniably hard, whether the subject is weight control for an individual or “wait control” in the emergency department. But even though it is easy to come up with excuses for allowing diets or change initiatives to slide, there are measurable rewards for adopting an approach that allows a person or an institution to set the right targets, achieve those goals and stay on track.
Chocking the Barriers to Change in Healthcare System.By.Dr.Mahboob ali khan Phd
Physician Engagement 2014
1. Physician Engagement…It Takes a Village
Physician engagement is critical to any healthcare organization. According to the
AMGA/Cejka Search Study, turnover costs are estimated at $1 million per physician
when active recruitment, bonuses, start-up, lost revenue, and internal costs for
interviewing and onboarding are considered. This does not include the possibility of
permanent market share loss; frequently, patients leave with their physicians. Losing
physicians can put the financial wellbeing of any healthcare organization at risk ;1
however, the cost of engagement reflected by turnover can be crippling to a small
healthcare organization. How can physician engagement be increased while
decreasing turnover? How can leadership learn to work better with physicians? Give
respect, ask for input, and communicate, communicate, communicate.
Adena Health System, located in Southeastern Ohio, employs 160 physicians in its
medical group. Before 2010, little thought was given to physician engagement. An
employee engagement survey, administered through Gallup, was measured and
reported annually. Action plans were implemented in areas where scores fell below a
certain grand mean; plans included increased mentoring opportunities for leadership.
Scores were expected to increase; however, efforts within our organization ended at
the staff level. Very little attention was given to the physicians, who Adena began
employing in 1998. Typically, if a physician left the health system, they were labeled
as “not the right fit”. It was a simple way of masking a growing problem—physician
engagement.
The 2010 physician engagement survey results showed us that 33% of our medical
group was “Actively Disengaged”, which meant they didn’t hesitate to refer to
physicians outside of Adena and were antagonistic toward Adena and administration.
Our “Fully Engaged” physicians (those who were very loyal and emotionally attached
to Adena) measured at 14%, or approximately 22 physicians. Although these survey
results were not bad, our attrition rate continued to grow. In 2010, we lost 16
physicians—more than 10% of our medical group. In 2012, we hit an all-time high,
losing 28 physicians in one year.
Understanding the Real Costs of Recruiting and Retaining Physicians, Lori Schutte, Recruiting1
Physicians Today, Volume 20, No. 3, May/June 2012
2. The 2012 survey reflected that 41% of our physician group was “Actively Disengaged”,
while our “Fully Engaged” group dropped to 8%. The results were alarming, but made
sense in context—we lost 28 physicians that “weren’t the right fit “during the year. In
order to determine the root cause of the physician disengagement trend, the
Physician Human Resources Director, Chief Learning Officer, and the lead physician
over engagement visited 28 practices and interviewed 98 physicians. After the survey
results were presented and explained, the dialogue began.
Through this process, we discovered many contributing factors to overall physician
disengagement. Physicians felt they had no input in regard to decisions being made
by administration; when decisions were made, very little context was given, and the
reasoning behind the decisions was not shared. Many physicians simply felt
disrespected by administration and by peers. The departure of 28 physicians within
a one-year period left several with a looming sense of fear—if they were unsure of
why a peer left, they often believed the move was involuntary—many suspected they
would be next.
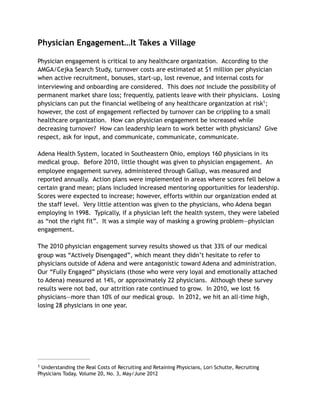
Clearly, communication was lacking. Additional reasons for disengagement given
during the interviews are outlined below:
Adena Physician Separation Rate
2005-2013
0.00%
20.00%
2005 2006 2007 2008 2009 2010 2011 2012 2013
2.86%
7.50%
5.04%
7.63% 8.27%
10.49%
15.17%
18.92%
8.00%
3. The results of the interview process allowed us to create a focused plan of action.
1. Create a Goal
Our first action item was to establish a goal and subsequently develop a plan
around physician attrition. For 2013, we set the goal at no more than 10%
attrition. We had to have something outside of the Gallup score by which to
measure our work; we measured and tracked our work throughout the year by
utilizing an A3 annual planning tool.
4. 2. Use Peer Support
Our second action item was to create a Provider Engagement Steering
Committee. This committee was comprised of staff-level physicians and one
leader. In addition, a Nurse Practitioner and CRNA were added in order to
represent our Advanced Practice Provider group. Meetings were held monthly.
Topics for discussion included the physician frustrations voiced in the
interviews, initiatives to assist with engagement, and a re-evaluation of the
physician evaluation tool. An anonymous email account was established for
physicians to send their concerns, which were then addressed through the
committee.
3. Leadership
Physician leadership became a new focus for us. In 2008, prior to our focused
approach to engagement, a structure for physician practices and subsequent
hierarchy was established. We asked various physicians to become medical
directors, division chairs and practice leads without giving them the tools
necessary for successful leadership. In response to our 2012 survey results,
standard operating procedures (SOP’s) were created for:
5. ▪ Physician leadership expectations
▪ Role clarity between the physician leader and administrative dyad
partner
▪ Communication
▪ The evaluation process
4. Communication Expectations
The interviews made it clear that we were not soliciting enough input, we were
not taking opinions into consideration, and we were doing more telling than
listening. Expectations were defined for meeting frequency for our physician
leaders; this included individual meetings with other leaders and monthly
division meetings with all division physicians and advanced practice providers.
5. Mentor the New Physicians
Newly-hired physicians were given mentors; to qualify as a mentor, a physician
needed experience within the Adena medical group, a reputation for being
actively engaged and productive, and higher service excellence scores.
Mentors were expected to reach out their new peers and offer assistance with
questions; additional support was given through the Provider Engagement
Steering Committee.
6. Utilize EQ (Emotional Intelligence)
A physician “at risk” list was established and kept highly confidential.
Physicians were added to the list for a variety of reasons. Many were identified
as possibly being unhappy because of living away from home/family. Others
were viewed as being anxious about compensation. Some were added for being
actively disengaged. Physicians on the list were identified by their physician
leaders, administrative directors or other leaders within the organization.
When a physician was identified, the Chief Learning Officer, a certified
Emotional Intelligence (EQ) coach, began working with that individual to assess
the need or potential gap. Through EQ coaching and behavior changes,
physicians were saved who would have been lost to the system otherwise.
By saving one physician at a time, Adena only lost 12 physicians in 2013. Although 12
is still too many, , we hit our goal of less than 10%; in fact, our attrition rate fell to 5%
in 2013 (a rate we hadn’t achieved since 2007). Our hard work also made us eligible
for the Gallup Great Workplace Award, which we won for our efforts in 2013.
6. Lessons Learned:
1. Focus on leadership and the development of physician leaders. They are
trained to diagnose and treat patients, not to lead.
2. Insist that physician issues have physician input. Decisions made solely by
administration will fail without the right input.
3. Stay connected with physicians in your organization. We all have issues, and
physicians are no different.
4. Communication is critical – it cannot be emphasized enough.
5. Transparency about performance is important. Success is dependent upon the
physicians. The more they know, the better.
6. Physician engagement has to be a focus for the entire leadership team,
particularly in the C-Suite. If the organization has an incentive for leadership,
ensure that engagement is a goal for all.
7. Success, at any level, begins with engagement. Without engaged physicians,
advanced practice providers, leaders, and employees, all other work is for
naught.
8. It takes a village. Depending upon the circumstances, it should be “all hands
on deck”. Issues addressed included communication between physician division
chairs and physicians, poor office space, difficulty with staff, and assistance
needed with Information Technology. Because we, as a system, declared
engagement a priority, we acted on each one.
We still have a long way to go to reduce our physician attrition rate. The “at risk” list
is still active, and we still utilize group efforts when it comes to saving a member of
our medical group. Within the next two years, engagement will be pulled through the
organization instead of being pushed. Engagement can never be optional.
Gail Games
Chief Learning Officer
Adena Health System
September, 2014