The document proposes a policy to establish universal primary healthcare in India through a decentralized community-based model. Key aspects include:
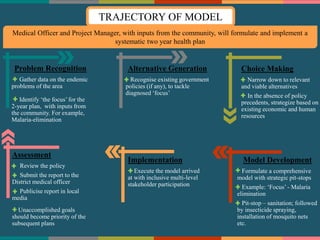
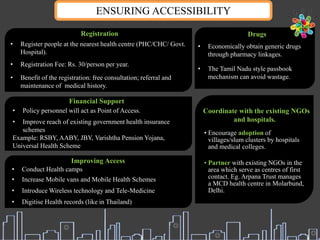
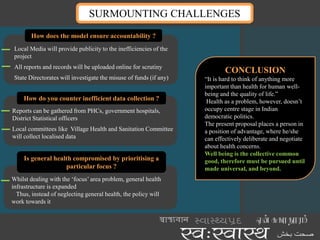
1) Developing area-specific 2-year health plans at the sub-district level to address priority health issues like malaria, with involvement from medical officers, staff, and community stakeholders.
2) Establishing incentives for community participation in health as well as career growth for medical professionals involved in implementing plans.
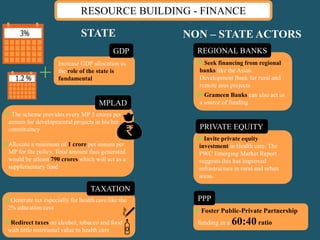
3) Mobilizing resources from various sources including government budgets, private partnerships, and financing institutions to strengthen infrastructure and ensure accessibility of healthcare for all.
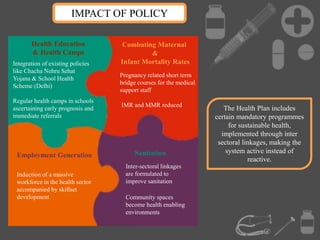
The model aims to improve health outcomes through inter-sectoral coordination and making primary healthcare systems proactive and sustainable.






















































































![PERI-PROSTHETIC FRACTURE NAIL-PLATE CONSTRUCT [NPC].pptx](https://cdn.slidesharecdn.com/ss_thumbnails/drarunkumardrmohamedashrafperiprostheticfrasturenail-plateconstructnpc-260209164459-7e9d15a1-thumbnail.jpg?width=640&height=640&fit=bounds)




