Definitions:
• Pharmacology:
Pharmacology: fromGreek; pharmakon, "poison or
drug in modern Greek"; and logia "Study of’’
Pharmacology can be defined as the study of the
effects of drugs on the functions of living systems
the study of substances that interact with living
systems through chemical processes, especially by
binding to regulatory molecules and activating or
inhibiting normal body processes.
the study of actions of drugs on the body
(pharmacodynamics) and the fate of drugs in the
body (pharmacokinetics).
3.
Drug:
a chemical agentwhich can affect living processes.
are chemicals administered to achieve a beneficial
therapeutic effect in a patient or for their toxic
effects on regulatory processes in parasites infecting
the patient.
4.
Clinical pharmacology:study of drugs as applied in
prevention, diagnosis and treatment of disease
Toxicology: branch of pharmacology involved in the
study of "undesirable" effects of drugs on biological
processes
5.
Indication: Anillness or disorder in which a specific
drug has a documented usefulness.
Contra- indication: A health condition/state in
which a particular drug is not used as it may cause
more harm e.g. aspirin is contraindicated in peptic
ulcers.
Drug Interactions: A situation whereby drugs
interacting with each other thereby altering each
other’s duration and magnitude of pharmacological
action.
Pharmacy: Branch of health science that deals with
preparation and dispensing of drugs.
6.
Idiosyncrasy: Inheritedabnormal response to drugs
mediated by genes. Response can be increased,
decreased or bizarre e.g. fast and slow acetylation
(breakdown) of isoniazid.
Iatrogenic Responses: These are responses produced
unintentionally during the treatment of client e.g.
Penicillins may cause hepatic toxicity;
Intolerance: Low threshold to normal
pharmacological action of a drug. A drug causes an
exaggeration of a normal pharmacological response
e.g. Morphine may cause coma instead of respiratory
distress which occurs with administration of a normal
dose.
7.
Bactericidal: asubstance that kills bacteria
Bacteriastatic: is a biological or chemical agent that
stops bacteria from growing or reproducing, while
not necessarily killing them
8.
Tolerance: Decreasedresponse to a drug as a result
of continuous exposure at the same dose or need to
increase the dose of a drug to achieve the same effect.
Half-life or Half time (t½): Time taken for plasma
concentration of a drug to fall by half or 50%
following its elimination from the body. It enables
one to maintain a steady state/critical plasma
concentrations of a drug in which there is maximum
therapeutic effects and minimum adverse effects. It
determines the frequency of drug administration.
9.
Dependence: Statearising from repeated periodic or
continuous administration of a drug that results in the
Person(s) feeling a desire or a compulsion to continue
using the drug and feeling ill if abruptly withdrawn or
an antidote is used.
Substances that cause dependence are taken to induce
good feelings, or avoid discomfort of their absence.
Potency: This is the amount (weight) of a drug in
relation to its effects e.g. if weight-for-weight drug A
has greater effect than drug B then drug A is more
potent than drug B.
10.
Receptors: Mostdrugs act by associating with
specific macromolecules in ways that alter the
biochemical or biophysical activities of the
macromolecules. The component of a cell or
organism that interacts with a drug and initiates the
chain of events leading to the drug’s observed effects,
(therapeutic or adverse is called a receptor.
Placebo: Any component of therapy that is without
specific biological activity for the condition being
treated e.g. inactive substance such as saline or
distilled water, usually used in clinical trials research
and for psychological treatments.
11.
Agonists: Theseare drugs that bind and activate
receptors because they resemble the natural
chemicals and produce the same effects as the natural
chemicals.
Antagonist (blockers): These are substances/drugs
that are sufficiently similar to the natural substance to
be recognized by the receptors and to occupy them
without activation thereby preventing (blocking) the
natural substance from exerting its effect. The
antagonists that have completely no activating effect
are called pure antagonist. Others exert low degree
activation and are called partial agonist.
12.
Pharmcokinetics: what thebody does to the drugs;
Also refers to the movement of drug into, through,
and out of the body:
comprises of:
–A: absorption
–D- distribution
–M: metabolism
–E: elimination/excretion
Pharmacodynamics: what the drug does to the body;
deals with mechanisms of action and drug effects in
the body
14.
A) Plants sources
Plants are an important source of chemicals that are
developed into drugs. Any part of the plant; including
leaves, roots and bark can be used.
Some of the active ingredients from plants used to
make drugs includes
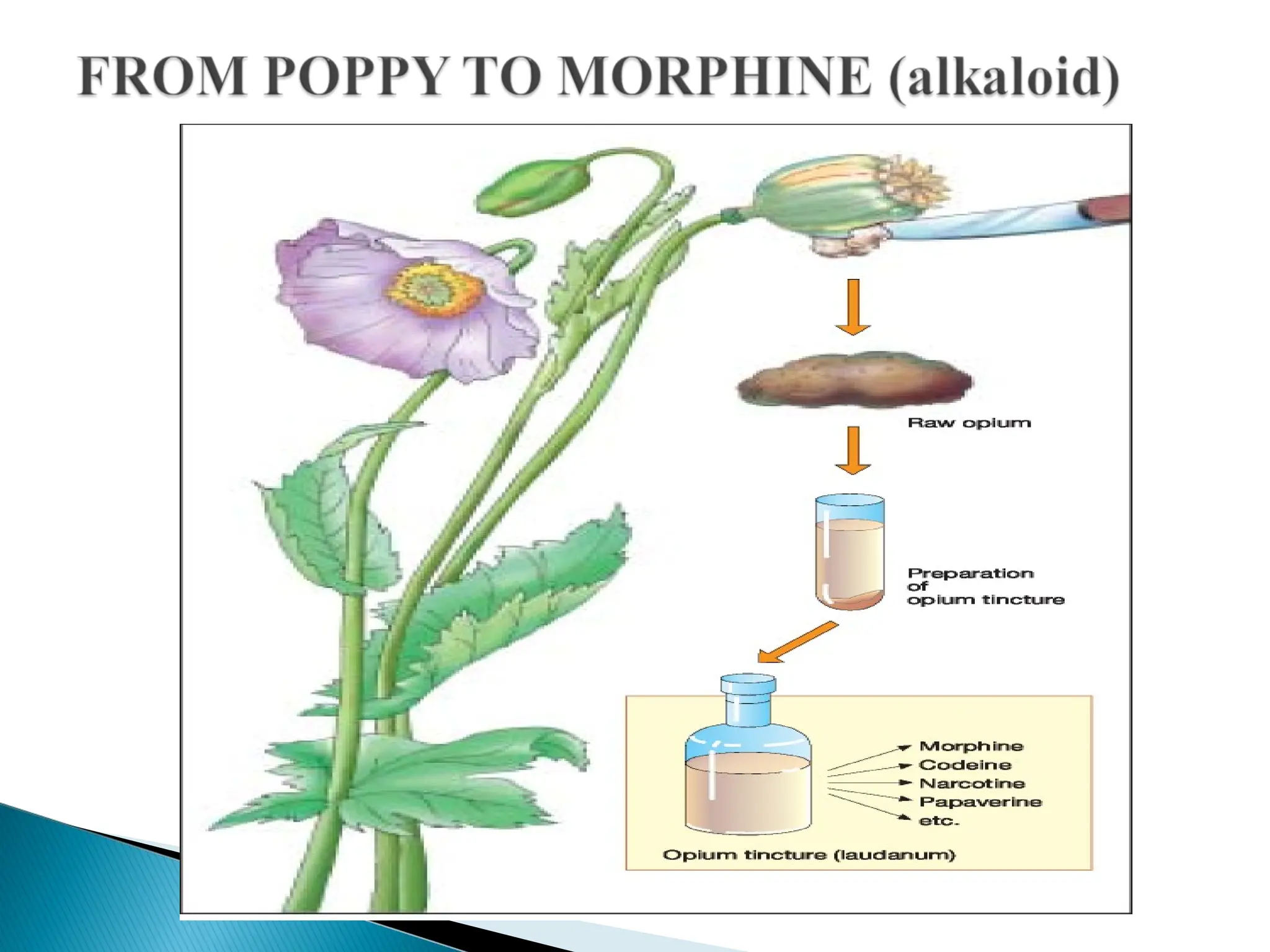
1. Alkaloids: Alkaloids are a group of naturally
occurring chemical compounds, that mostly contain
basic nitrogen atoms.
15.
Examples ofdrugs derived from alkaloids include:
Atropine, cocaine, quinine, codeine and morphine.
2. Glycosides: These are Digitalis products e.g.
digoxin, digitoxin which are gotten from Digitalis
Purpurea or foxglove plant.
3. Oils: These can be volatile oils like peppermint,
spearmint, menthol, cinnamon, lemon camphor.
These have pleasant fragrance and evaporate easily.
4. Resins:(Hydrocarbon secretion of many plants) the
most common resin is benzoin which is used as an
antiseptic.
17.
These aremainly used to replace human chemicals
that are not produced adequately due to disease or
genetic problems e.g. insulin from pancreases of
cows and pigs.
Other substances gotten from animals include
thyroid drugs (from animal thyroid) and growth
hormone preparation from animal hypothalamus.
18.
Salts ofvarious elements can have therapeutic effects
in the human body e.g. Aluminum (used as antacids),
Fluoride (used to prevent dental cavities and
osteoporosis), Gold (used for rheumatoid arthritis),
iron (used for Anemia) and potassium (used in K+
supplements).
D) Synthetic Sources
Many drugs are developed synthetically using
genetic engineering to produce chemicals that have
therapeutic effects e.g quinolones
19.
1. Curativepurposes- This could be primary therapy
e.g. in treating bacterial infections.
2. Suppress, signs and symptoms, hence improve
quality of life without attaining cure e.g. anti
diabetics.
3. Preventive/ prophylaxis- This could be primary
e.g. use of vaccines to prevent one from getting a
disease or secondary to stop progression of an
already existing disease.
4. Diagnosis of disease- For instance the use of
tuberculin test to diagnose PTB
20.
Drugs maybe administeredthrough various routes
including:
1. Enteral route- This is administration of drugs along
any portion of the GIT includes Oral, Rectal , Buccal .
2. Parenteral route – This is administration of drugs
through other routes outside GIT e.g. subcutaneous
route, intramuscular route, intravenous, intrathecal and
intraspinal.
3. Pulmonary route. This is mainly through
inhalation.
4. Topical. This is mainly application on the skin
21.
IV ROUTE
Advantage
Youcan deliver drugs in large amounts,
you will have 100 percent bioavailability.
Disadvantage
Can't reverse a toxic dose, requires specialized personnel.
May be expensive.
22.
Subcutaneous Advantage
Absorptionis slow but complete.
This route is improved by massage or heat.
Vasconstrictor may be added to decrease absorption of
a anesthetic agent, therefore prolonging its effect at the
site of interest
SC Disadvantage
This route may be painful ,
irritant drugs can cause local tissue damage.
Small doses limit use
23.
Oral Advantages
Convenient
economical,
non invasive often safer route,
requires no special training
Oral Disadvantages
drug delivery is usually incomplete.
Highly dependent on patient compliance .
Increased drug- drug, and drug- food interactions .
Drugs are exposed to first pass effect
24.
Buccal/ Sublingual Advantages
In this route of administration, the liver is bypassed ,
and bioavailability is higher.
This type of administration has rapid absorption
Buccal / Sublingual Disadvantages
Holding the dose in the mouth is an inconvenience .
If any of the drug is swallowed it will then be subject
to the first pass effect.
25.
Intramuscular Advantages
largervolume than sc, can be given by IM .
A depot or sustained release effect is possible with IM
injections ( some penicillin)
Intramuscular Disadvantages
Requires trained personal ,
the site of injection will influence the absorption.
Absorption is erratic , especially for poorly soluble
drugs (diazepam and phenytoin ).
The solvent may be absorbed faster than the drug
causing precipitation)
26.
Intra arterial
forcancer chemotherapy to maximize drug
concentration at the tumor site
Rectal Advantages
By passes liver . It has a reduced first pass effect .
This route is useful if patients cant take drugs orally or
with young children ( example diazepam )
Rectal Disadvantages
Erratic absorption-
27.
Drugs aremanufactured or prepared in various forms.
These forms reflect to a great extent the route of
administration of the particular drug. Preparations
includes
1. Solids e.g. Tablets, Caplets, Capsules, Troches
(lozenge).
a. Tablets -Tablet – a powdered drug compressed into a
small hard disc, some are readily broken along a scored
line, others are enteric coated to prevent them from
dissolving in the stomach
b. Caplet – a solid form, shaped like a capsule, coated
and easily swallowed
28.
C .Capsule;- a gelatinous container to hold a drug in
powder, liquid or oil form.
D. Lozenge (troche) – a flat, round or oval
preparation that dissolves and releases a drug when
held in the mouth.
2. Liquids e.g. Syrups, Elixirs, Suspensions, Emulsions .
a. Syrup – an aqueous solution of sugar often used to
disguise unpleasant tasting drugs
b. Elixir – a sweetened and aromatic solution of alcohol
used as a vehicle for medicinal agents
29.
Suspensions- liquidwith solid particles suspended
Emulsions mixture of two or more liquids in which one is
present as droplets.
3. Topical application drugs; -Creams/ointments/gels
a. Creams – a non-greasy, semisolid preparation used on the skin.
It is an emulsion of oil and water in approximately equal
proportions.
b. Ointment (salve, unction) – a semisolid preparation of one or
more drugs used for application to the skin and mucous
membrane
c. Gel or jelly – A clear or translucent semisolid that liquefies
when applied to the skin
30.
4. Aerosals andinhalation drugs.
Aerosol spray or foam – a liquid, powder or foam
deposited in a thin layer on the skin by air pressure.
Inhalation drugs are inhaled.
5. Pessaries and suppositories
Suppository – one or several drugs mixed with a firm
base such as gelatin and shaped for insertion into the
body (e.g. the rectum); the base dissolves gradually at
body temperature, releasing the drug
A pessary is a medical device inserted into the vagina,
either to provide structural support, or as a method of
delivering medication
31.
After achemical that might have a therapeutic value is
identified it must undergo a series of scientific tests to
evaluate its actual therapeutic and toxic effects.
This process is controlled by legally established
bodies’ e.g. Pharmacy and Poisons Board and Food &
drug administration (FDA) in Kenya and US
respectively.
For every 100,000 chemicals that are identified as
being potential drugs, only 5 end up being marketed as
drugs.
32.
Before receivinglegal approval to be marketed to the
public, drugs must pass through several sequential
stages of development including:
Pre-clinical trials Phase I Phase II
Phase III Phase IV
33.
Pre-Clinical studiesin animals
This phase involves testing of the drugs on laboratory
animals to determine if they have presumed effect in
living tissue and evaluate any adverse effects.
At the end of these trials, some chemicals may be
discarded for the following reasons:
1. They may lack therapeutic activity
2. They may be too toxic
3. If discovered to be teratogenic – Cause adverse effects
on fetus
4. True safety margin may be too small for chemical use.
Those found to have therapeutic effects and reasonable
safety margins pass to the next stage of drug evaluation
34.
Phase I:Clinical pharmacology
In this first phase, human volunteers, usually 20- 50
(healthy volunteers or volunteer patients depending on
the class of drug and its safety) are used to test the drug.
In this phase the pharmacokinetics and pharmacodynamic
of the drug are tested. This is done in tightly controlled
studies by specially trained clinical investigators.
During this phase toxicity and therapeutic effects are
further tested. At this stage, drugs may be rejected for the
following reasons:-
1. Lack of therapeutic effect in man
2. They may have severe adverse effects and/or be too toxic
3. If discovered to be Teratogenic.
35.
In thisphase, clinical investigators test drugs in patients
who have the disease that the drug is meant to treat.
Usually 100- 200 patients are involved in the study.
Pharmacokinetics and pharmacodynamics are determined
as well as Dosing requirements and efficacy of the drug
at the given dose.
After Phase II studies, a drug may be removed from
further investigation in case of the following;
1. If the drug is less effective than anticipated.
2. If it is discovered to be too toxic when used in humans.
3. If the drug is likely to produce unacceptable adverse
effects
36.
4. Drugs withlow benefit- risk ratio i.e. therapeutic
benefits do not outweigh the risk of potential adverse
effects.
5. If it is not more effective than other drugs already in
the market making the cost of continued research
uneconomical to the company.
Drugs that show promise of a therapeutic agent go to
phase III
37.
After thesecond phase, the drugs are taken to the
third phase whereby they are used in a vast clinical
market. 300 – 3,000 patients are involved in the
study. Prescribers are informed of all known actions
of the drug and precaution to take for its safe use. It’s
important to note that unexpected responses may
occur in wide use of a drug. Prescribers observe
patients closely for drug adverse effects and also
therapeutic effects.
38.
Once theregulatory body is satisfied that a drug has
undergone phase III, then it approves the marketing
of the drug. Duration of drug development and
approval is approximately 5-6 years but this duration
may be shortened if the drug is needed urgently.
39.
After adrug is approved for marketing, it enters a
continuous evaluation phase (phase IV) which goes
on for unspecified duration of time.
Prescribers are expected to report to the regulatory
bodies any unexpected effects which then evaluate
this information.
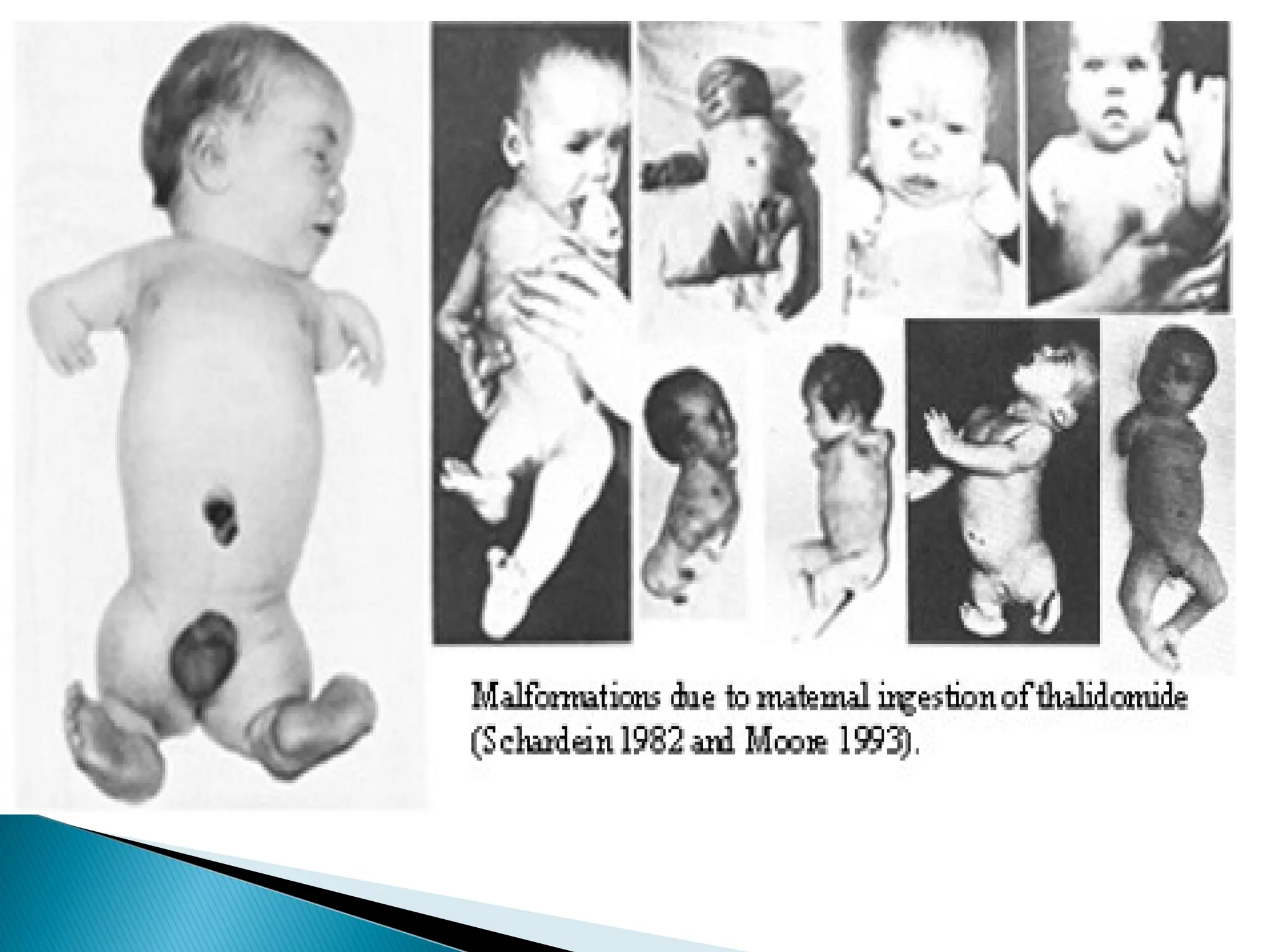
After wide distribution some unexpected effects may
occur and the drug may be withdrawn from the
market e.g thalidomide.
41.
Drug nomenclatureis the act of creating names for
a drug or other pharmaceutical substance.
Every drug has at least three names.
First, there's the chemical name, then there's the
non-proprietary name (generic name), and then
there is a brand name or Trade name (sometimes
more than one, if it's produced by more than one
company).
42.
Chemical nameis the name used by the organic
chemist to indicate the chemical structure of the drug.
Chemical names are quite long and difficult to
remember, spell, and pronounce as most of the organic
drugs are complex molecules. This name is not suitable
for routine use by medical professionals or common
people. However, this name is very helpful for the
discovery of new compounds.
43.
Medical professionalschoose the non-proprietary
name for its simplicity. It is always concise and
meaningful. For example, the word methylnitro is
condensed to metro and nidazole (Metronidazole)
The non-proprietary names are chosen by official
agencies including;
International Non-proprietary Names (INN)
British Approved Names (BAN)
United States Approved Names (USAN)
FDA
44.
This isshorter, simpler, easier to remember and most
frequently used. A drug can have several trade
names.
For example GlaxoSmithKline uses its
bronchodilator drug as ventolin instead of the non-
proprietary name salbutamol.
Different pharmaceutical companies market the same
drug with different trade names which may produce a
lot of confusion.
45.
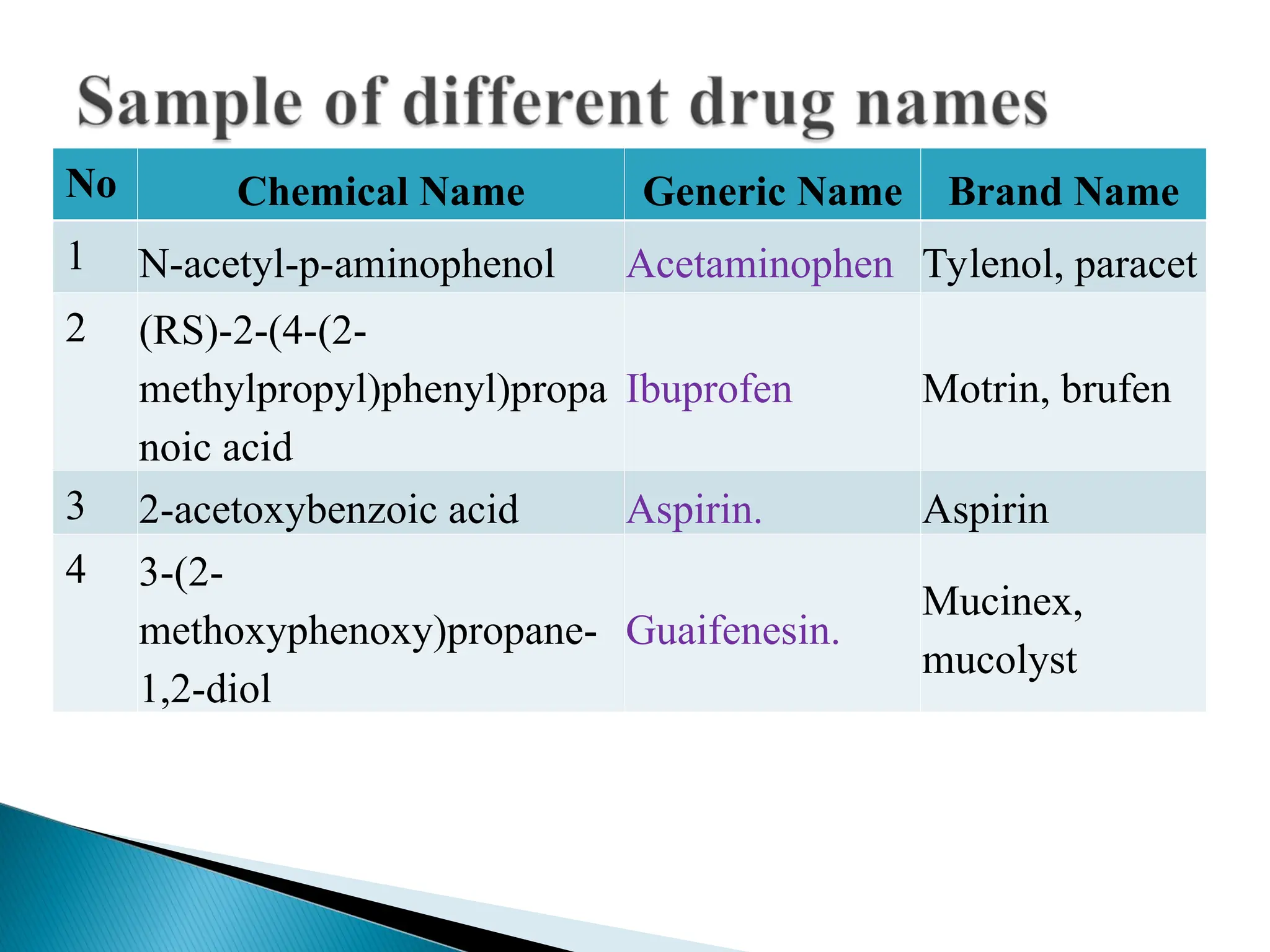
No Chemical NameGeneric Name Brand Name
1 N-acetyl-p-aminophenol Acetaminophen Tylenol, paracet
2 (RS)-2-(4-(2-
methylpropyl)phenyl)propa
noic acid
Ibuprofen Motrin, brufen
3 2-acetoxybenzoic acid Aspirin. Aspirin
4 3-(2-
methoxyphenoxy)propane-
1,2-diol
Guaifenesin.
Mucinex,
mucolyst
Editor's Notes
#12 Pharmacokinetics refers to the movement of drug into, through, and out of the body—the time course of its absorption, bioavailability, distribution, metabolism, and excretion
Pharmacodynamics, described as what a drug does to the body, involves receptor binding, postreceptor effects, and chemical interactions.
#19 Tuberculin is a glycerol extract of the tubercle bacillus.




















![General pharmacology modified__ppt[1]](https://cdn.slidesharecdn.com/ss_thumbnails/generalpharmacologymodifiedppt1-210322102730-thumbnail.jpg?width=640&height=640&fit=bounds)

















































