Download to read offline

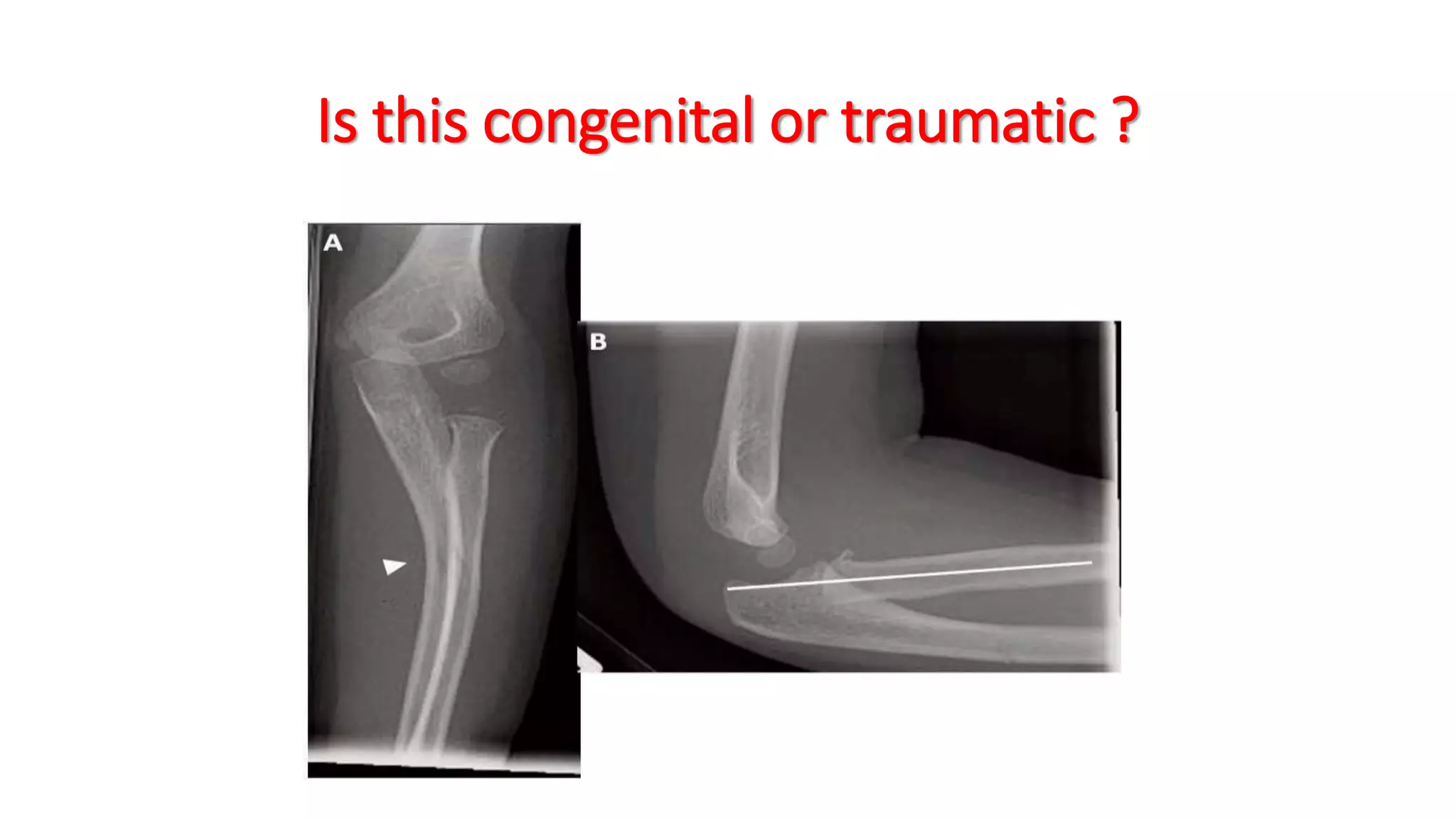































The document discusses pediatric radial head dislocation, highlighting the importance of differentiating between congenital and traumatic cases, as well as isolated and Monteggia dislocations. It emphasizes radiological assessment criteria, including anatomical relationships of ossification centers, and outlines various surgical and conservative treatment options for both congenital and traumatic conditions. Additionally, it addresses complications associated with surgical interventions and reinforces the need for individualized treatment planning.



































































