This document describes the development and implementation of a tool called the "Sunrise Claw" to improve the process of capturing sunrise projection x-rays of knees at an orthopedic clinic. The tool was designed to improve patient comfort, imaging quality, and workflow efficiency by allowing x-rays to be taken by a single technician without needing assistance holding the x-ray plate. Testing showed the tool reduced imaging time and improved outcomes. After further refinements, the Sunrise Claw was finalized and fully implemented for sunrise knee x-rays.










![PDSA- Orthopedics Faculty Clinic (OFC)-RADIOLOGY SUNRISE TOOLING
It was reported in Today (2012) that total knee replacements are increasing-Over 600,000 Yearly in US! Compared to
1999, total knee replacements have doubled (100% increase), to more than 600,000 per year. “On average, we take 1
[million] to 2 million steps per year. That’s a lot of back and forth on that hinge. And patients who are younger and
active can put significant force on that,” said Dr. Hanosh orthopedic surgery at the University of New Mexico in
Albuquerque. “But in terms of the value that you get from the surgery in terms of improvement in quality of life, this is
one of the best ways we can use our health care dollars.”
The sunrise view is a commonly requested x-ray view at Orthopedics Faculty Clinic (OFC). All new and follow-up total
knee arthroplasty (TKA) patients at Orthopedics Faculty Clinic require AP, Lateral, and Sunrise x-ray views. Due to the
increasing patient total knee arthroplasty patient volume, and a directive to improve clinic flow and to reduce operating
cost, tooling was selected to aid in improving radiology imaging services to meet these demands.
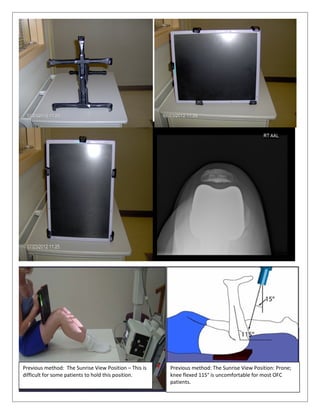
The Sunrise Claw tool](https://image.slidesharecdn.com/a13b5549-6ca9-45c2-905f-3aaa1efd4277-160823172248/85/PDSA-Sunrise-tooling-10-12-320.jpg)



















































