Downloaded 49 times


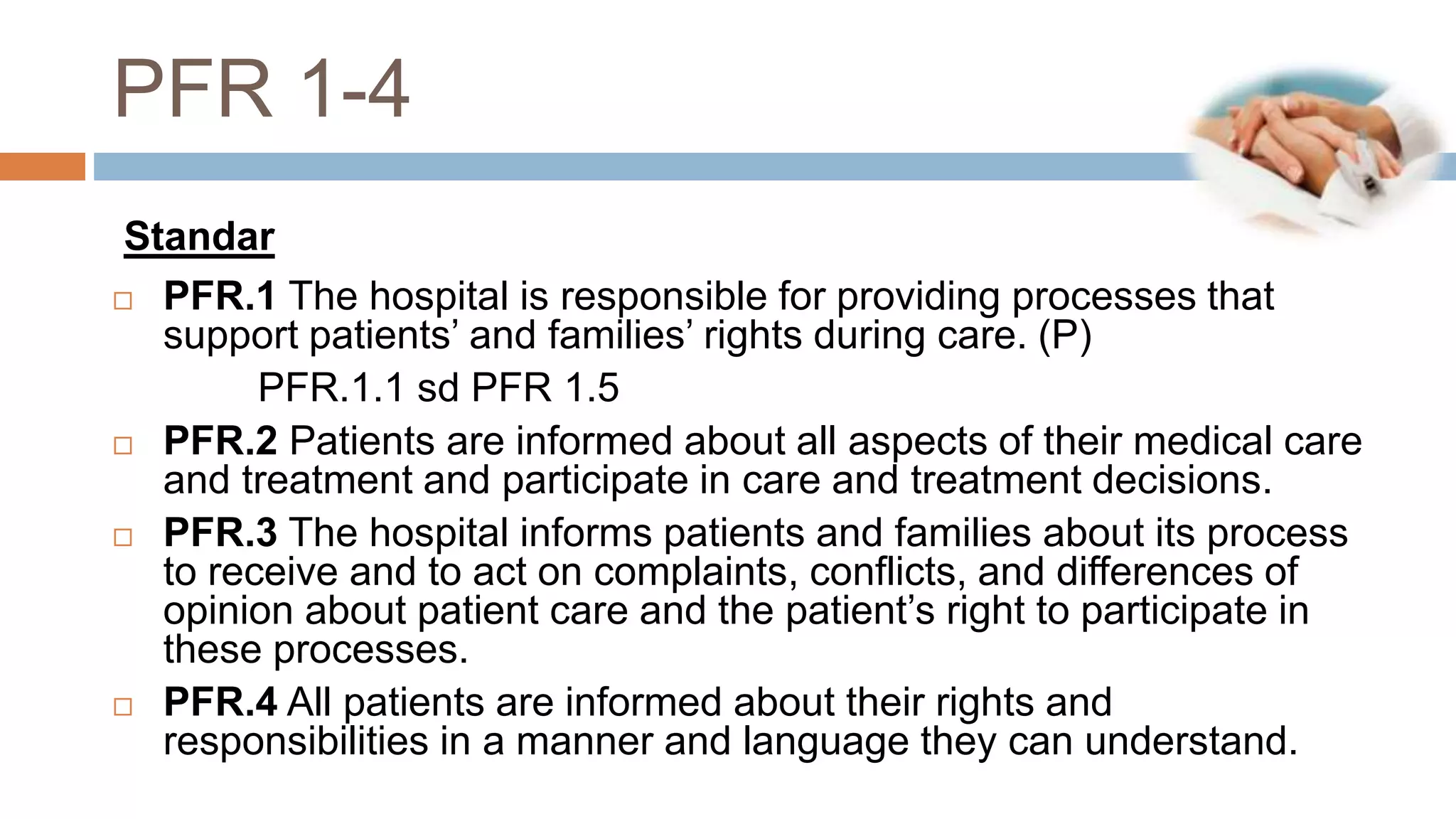




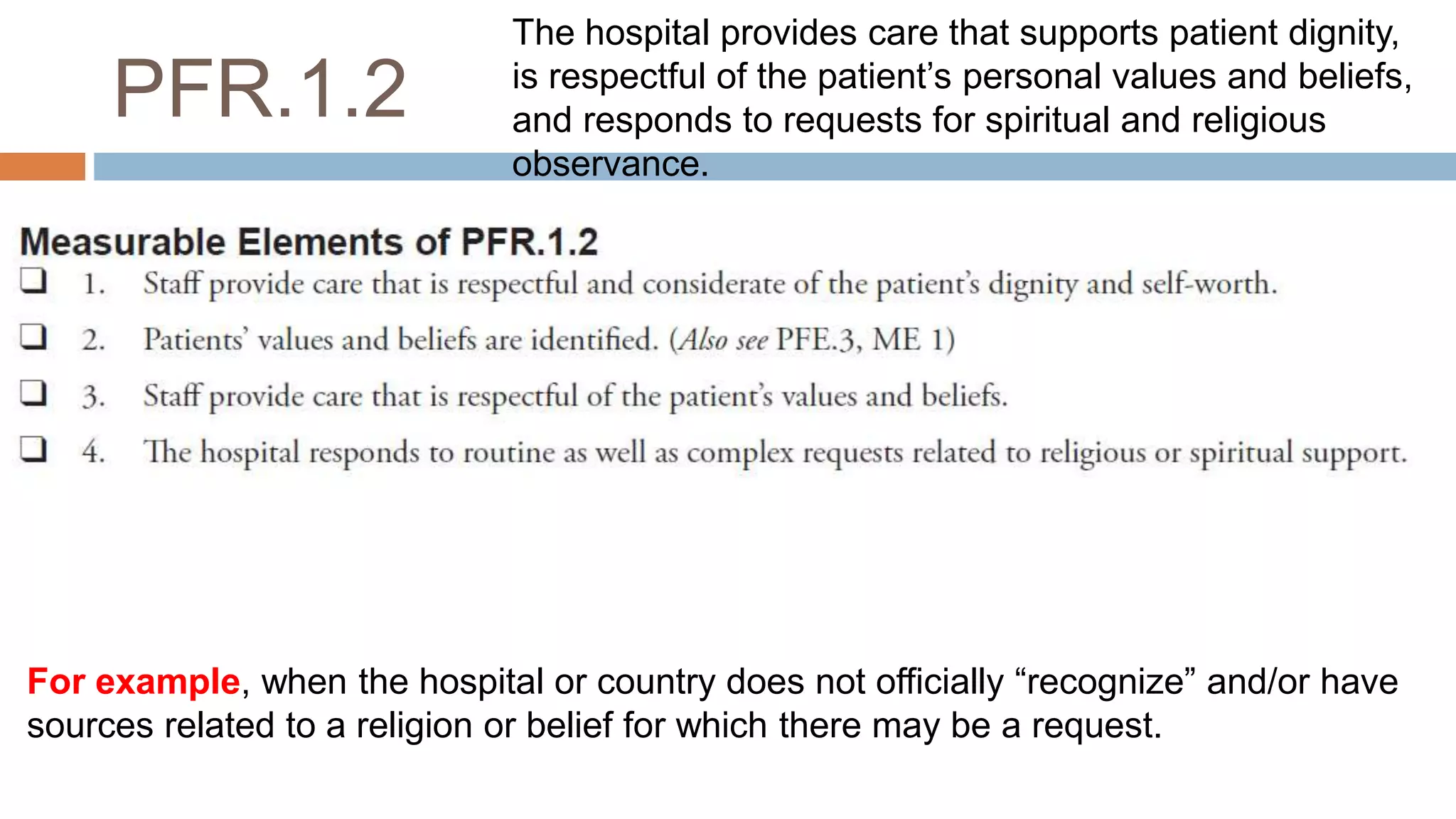


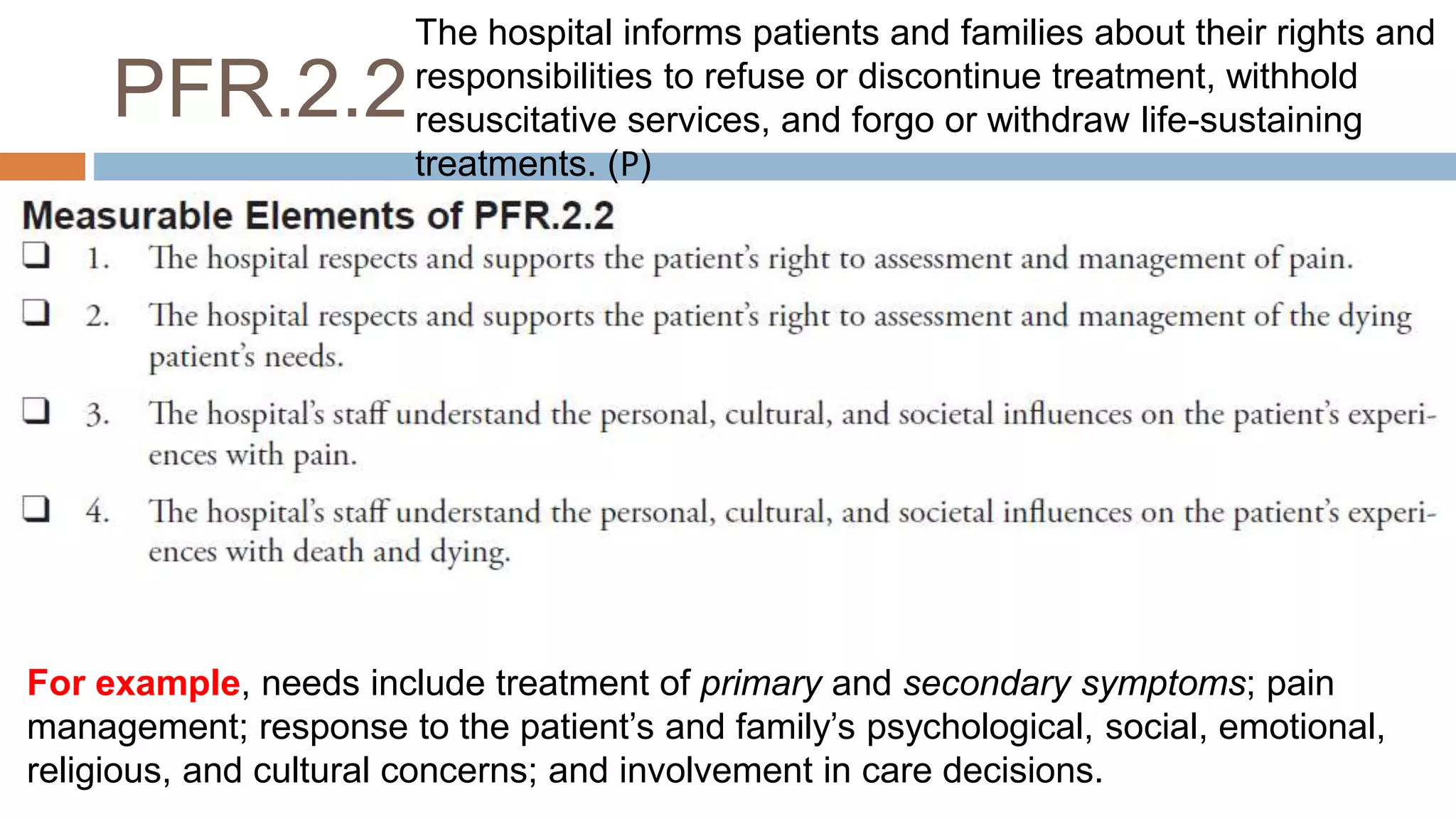
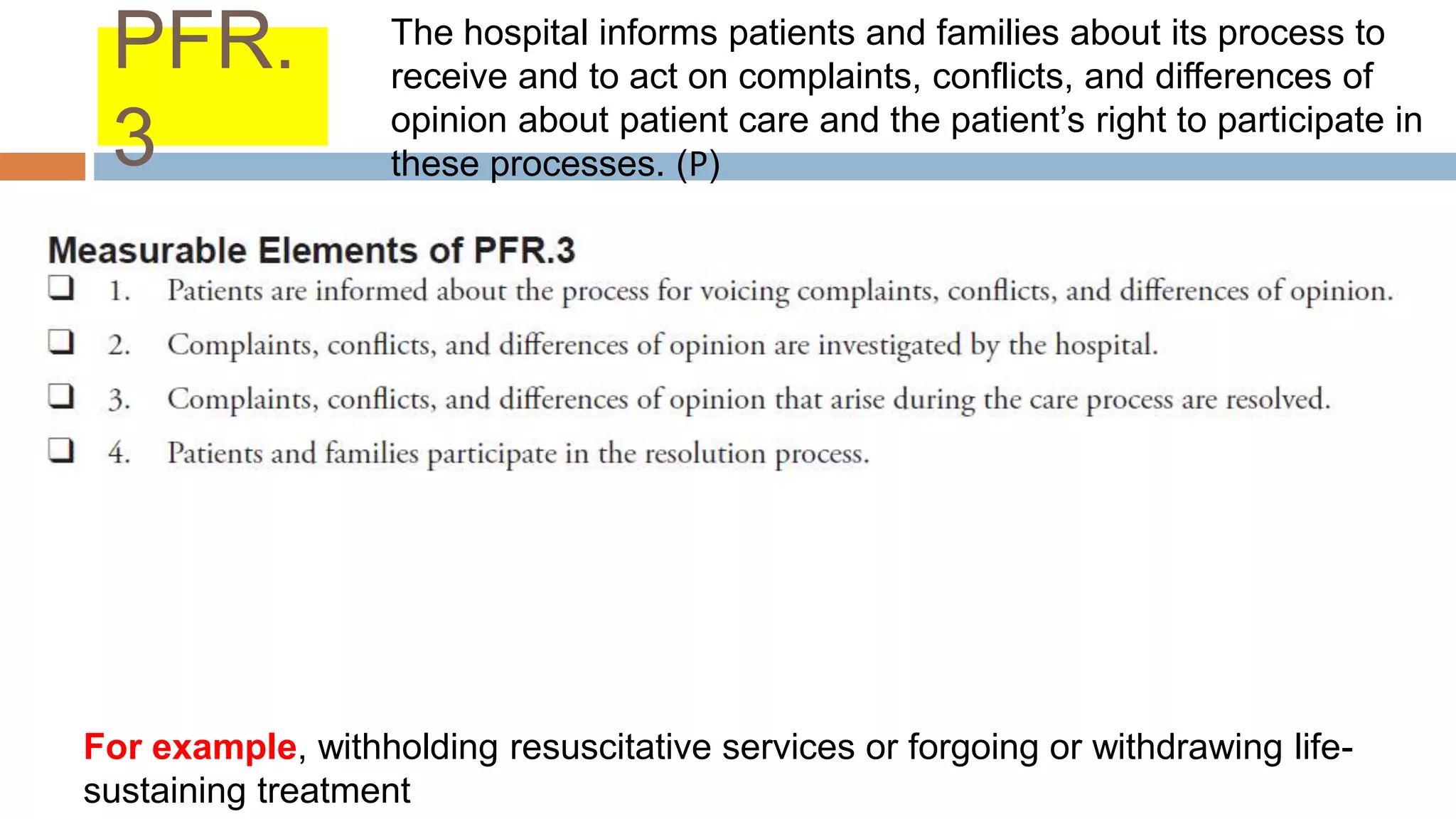




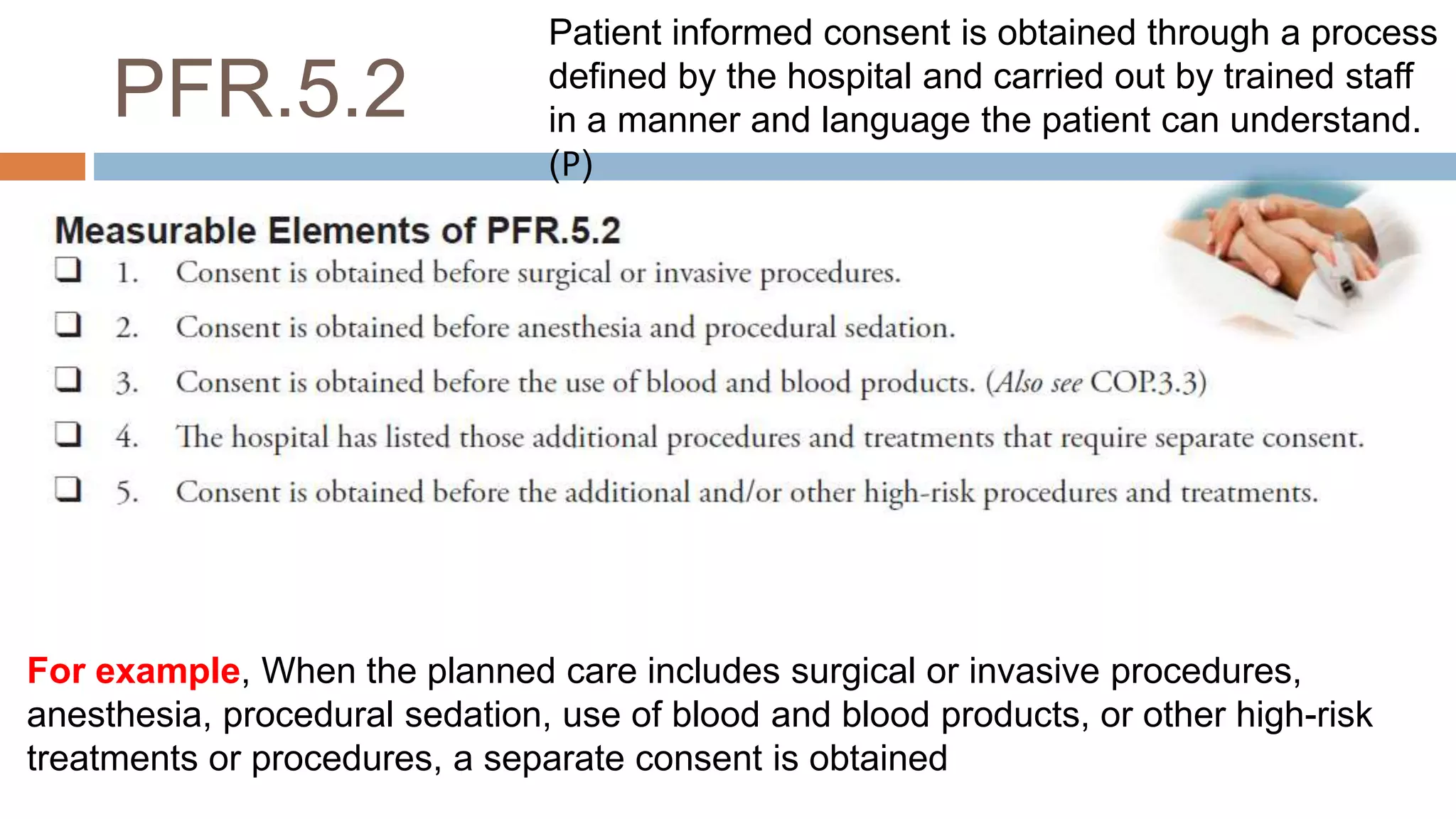


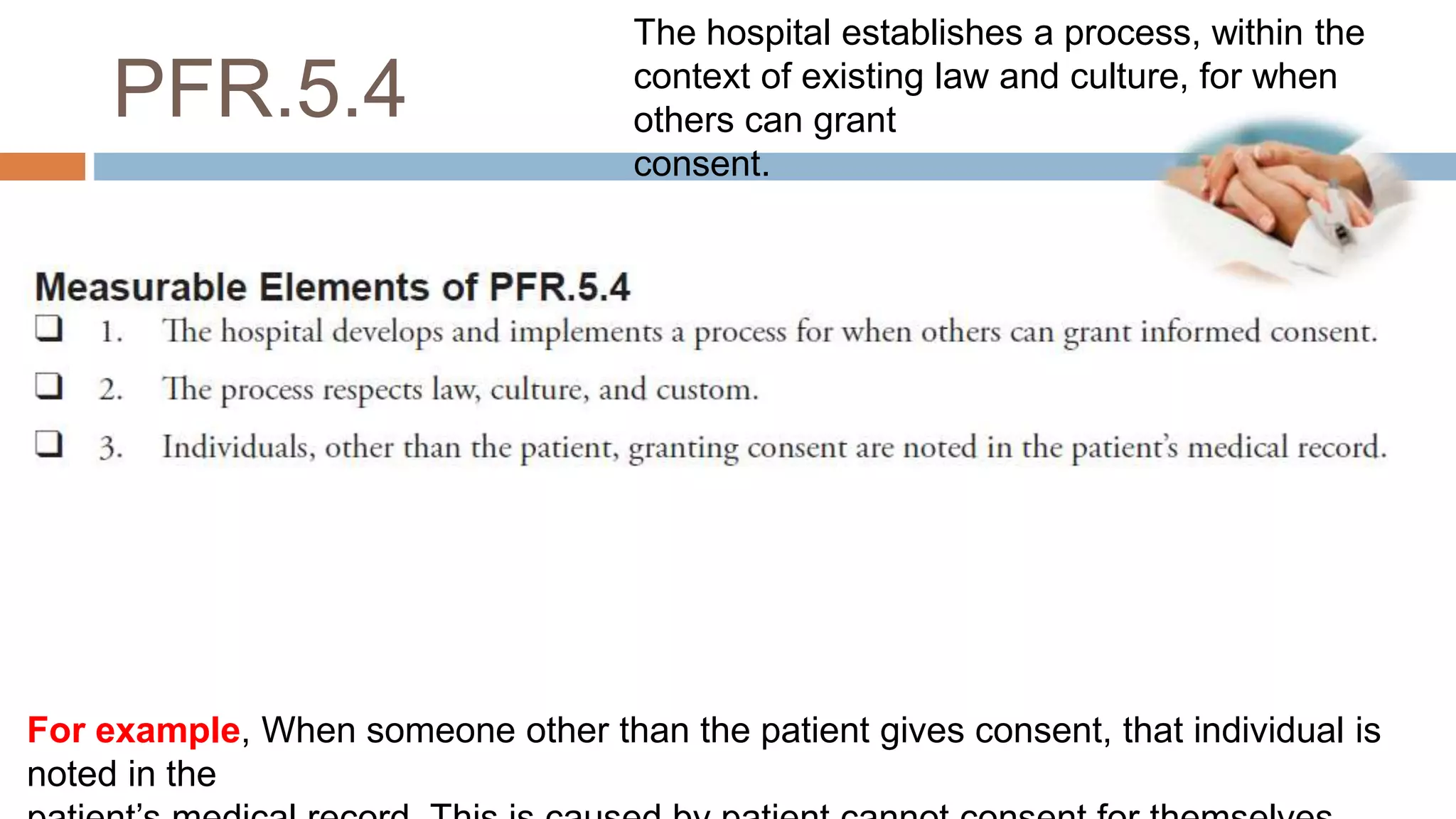





The document outlines standards for patient and family rights (PFR) at a hospital. It includes 6 standards with explanations and examples. Standard 1 states the hospital is responsible for providing processes that support patients' and families' rights during care, such as reducing barriers to access, respecting privacy and dignity, and protecting patients. Standard 2 requires informing patients about all aspects of their care and treatment and allowing them to participate in decisions. Standard 3 discusses informing patients about processes for complaints. Standard 4 requires informing patients of their rights and responsibilities in a way they understand. Standards 5 and 6 cover obtaining informed consent and informing patients about organ donation.



































































