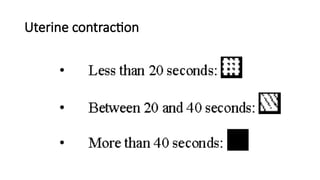
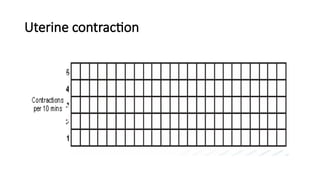
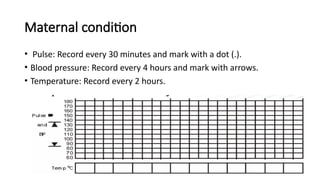
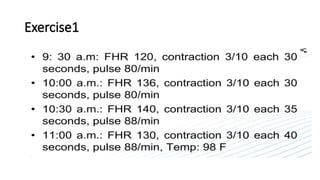
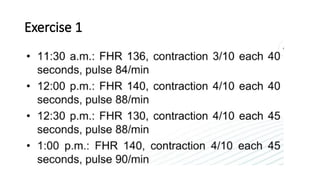
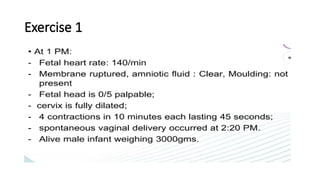
partograph (or partogram) is a crucial, cost-effective, and standardized visual tool used to monitor the progress of labor and the health of the mother and fetus, designed to detect abnormal labor early. It plots key data—primarily cervical dilation, fetal heart rate, and uterine contractions—against time to identify when interventions, such as augmentation or referral, are require




























































![CTEV [ clubfoot] DR ARUN LAL ,DR MOHAMED ASHRAF travancore medical college k...](https://cdn.slidesharecdn.com/ss_thumbnails/ctevclubfootdrarunlaldrmohamedashraftravancoremedicalcollegekollamkeralaindia-260208063247-18fc466c-thumbnail.jpg?width=640&height=640&fit=bounds)




