Definition
• Paget’s diseaseof bone (PDB) is a chronic
disorder of bone remodeling characterized by
excessive and disorganized bone turnover,
leading to structurally weak and deformed
bones.
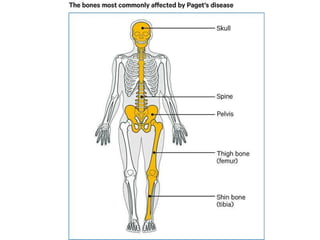
• Common sites: Pelvis, skull, spine, femur,
tibia.
5.
Pathophysiology
• • Excessiveosteoclastic activity Increased bone
→
resorption
• • Compensatory osteoblastic activity Disorganized bone
→
formation
• • Formation of woven bone (poorly mineralized,
structurally weak)
• • Increased vascularity Risk of high-output cardiac failure
→
• Key Pathological Hallmark: Mosaic pattern of lamellar bone
on histology
6.
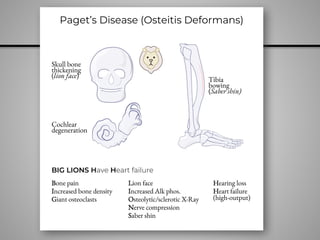
Clinical Features
• •🦴 Bone pain – Most common symptom
• • 📏 Bone deformities – Bowing of long bones, skull
enlargement (frontal bossing)
• • ⚡ Increased fracture risk – Pathologic fractures,
chalk-stick fractures
• • 🎧 Hearing loss – Due to skull involvement and
compression of CNVIII
• • 🔺 Increased warmth over affected bones – Due
to hypervascularity
• • 💓 High-output cardiac failure (rare) – Due to
increased AV shunting
8.
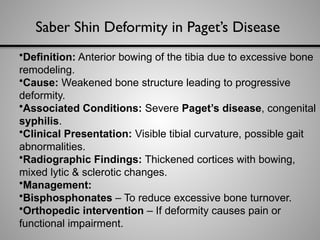
Saber Shin Deformityin Paget’s Disease
•Definition: Anterior bowing of the tibia due to excessive bone
remodeling.
•Cause: Weakened bone structure leading to progressive
deformity.
•Associated Conditions: Severe Paget’s disease, congenital
syphilis.
•Clinical Presentation: Visible tibial curvature, possible gait
abnormalities.
•Radiographic Findings: Thickened cortices with bowing,
mixed lytic & sclerotic changes.
•Management:
•Bisphosphonates – To reduce excessive bone turnover.
•Orthopedic intervention – If deformity causes pain or
functional impairment.
9.
Diagnosis - LabFindings
• • 🧪 Labs:
• - Alkaline phosphatase (ALP) (marker of bone
↑
turnover)
• - Normal calcium, phosphate, and PTH
• - Urinary hydroxyproline (bone resorption marker)
↑
• • 🎨 Imaging:
• - X-ray:Thickened cortices, mixed lytic & sclerotic
lesions
• - Bone scan: Increased uptake in affected bones
10.
Lab Findings –Detailed Explanation
• 1. Serum Alkaline Phosphatase (ALP) – 🔑 Key Marker
• - Elevated in active disease (due to increased osteoblastic activity)
↑
• - ALP correlates with disease burden & activity
• - Can be normal in early/monostotic disease
• Clinical Correlation:
• - High ALP + normal calcium & phosphate = Paget’s disease
• - High ALP + high calcium = Consider hyperparathyroidism, malignancy
• 2. Calcium and Phosphate – Normal Levels
• - Serum calcium = Normal (unlike primary hyperparathyroidism or
malignancy)
• - Serum phosphate = Normal (not a phosphate-related disorder)
• - Calcium only if immobilization or secondary hyperparathyroidism
↑
11.
• 3. UrinaryMarkers of Bone Resorption
• - Urinary Hydroxyproline (Released during collagen breakdown)
↑
🟢
• - Urinary N-telopeptide (NTX) & C-telopeptide (CTX) (Bone matrix
🟢 ↑
degradation)
• 4. BoneTurnover Markers
• - Serum C-terminal telopeptide (CTX) – Marker of osteoclast activity
🟢 ↑
• - Procollagen type 1 N-terminal propeptide (P1NP) – Marker of
🟢 ↑
osteoblast activity
• - Both elevated in active disease and decrease with effective treatment
• 5. Parathyroid Hormone (PTH) –Typically Normal
• - PDB does not directly affect PTH
• - PTH only in secondary hyperparathyroidism (e.g., due to vitamin D
↑
deficiency)
12.
Management
• • 💊First-line: Bisphosphonates (Zoledronic
acid,Alendronate) – Inhibit osteoclast activity
• • 💉 Calcitonin: Used if bisphosphonates
contraindicated
• • 🩼 Pain management: NSAIDs, physical
therapy
• •
️ 🛠️Surgical intervention: For fractures,
deformities, or severe arthritis
13.
Orthopedic Surgery/Intervention inPaget’s
Disease (Including Saber Shin Deformity)
• Orthopedic intervention is considered when
Paget’s disease causes severe deformities,
fractures, or functional impairment.The goals
are to relieve pain, correct deformities, and
restore function.
14.
1. Indications forSurgery
• ✅ Severe bone deformities (e.g., saber shin
deformity) causing pain or mobility issues
✅ Pathologic fractures (e.g., chalk-stick
fractures) that fail to heal conservatively
✅ Severe arthritis (secondary osteoarthritis
from bone misalignment)
✅ Spinal involvement causing nerve
compression (spinal stenosis)
✅ Osteosarcoma (rare complication) requiring
tumor resection
15.
2. Surgical Procedures
🔹Osteotomy (Bone Cutting & Realignment):
• Used for severe saber shin deformity to straighten the
tibia
• Bone is cut, repositioned, and fixed using plates, screws, or
rods
• Requires post-op immobilization and rehabilitation
🔹 Fracture Fixation (Internal Fixation):
• Plates, screws, or intramedullary rods used to stabilize
pathologic fractures
• Needed due to poor bone quality and delayed healing in
Paget’s
16.
Joint Replacement (Arthroplasty):
•Total knee or hip replacement if severe
arthritis develops
• Common in long-standing disease affecting weight-
bearing joints
🔹 Spinal Decompression Surgery:
• Performed if Paget’s disease causes spinal
stenosis with nerve compression
• Laminectomy or spinal fusion may be done
17.
3. Pre- &Post-Surgical Considerations
✅ Pre-Surgery:
• Optimize bone health with bisphosphonates (reduces
bleeding risk from hypervascular bone)
• Evaluate bone quality with imaging (X-ray, CT, MRI)
✅ Post-Surgery:
• Rehabilitation & physiotherapy for mobility recovery
• Pain management (NSAIDs, physical therapy)
• Monitor for complications (delayed healing, implant
failure, infection)
18.
Key Takeaways
• ✅Paget’s disease = Isolated elevated ALP with normal calcium
& phosphate
• ✅ Most common symptom = Bone pain
• ✅ Classic X-ray findings = Mixed lytic & sclerotic bone lesions
• ✅ Best initial treatment = Bisphosphonates
• ✅ Complications = Fractures, osteosarcoma (rare), hearing
loss, cardiac failure
• 🔑 ExamTip: Paget’s disease is often an incidental finding on
labs (isolated ALP in an older patient).Always correlate with
↑
symptoms & imaging!