Download to read offline


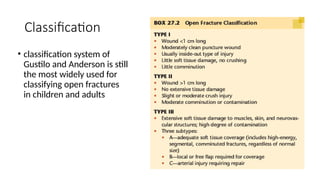


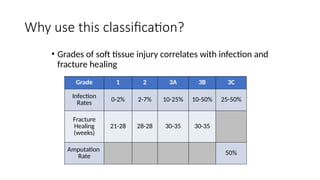
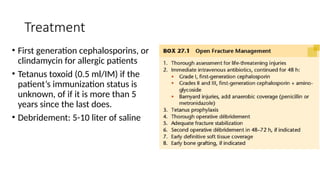
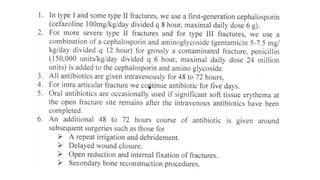
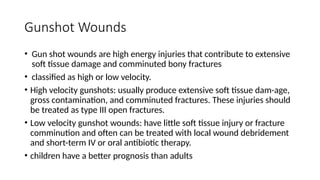
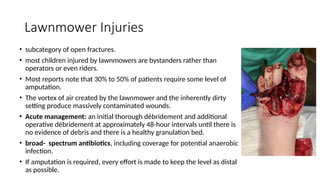

Open fractures are classified by communication with the environment and can lead to significant soft tissue damage, especially in high-energy traumas like gunshot wounds and lawnmower accidents. Management differs between children and adults primarily in healing rates and infection risk, with a common classification system being Gustilo and Anderson, which correlates soft tissue injury grades to infection and healing rates. Treatment often includes antibiotics, debridement, and, in severe cases, amputation, particularly in the presence of extensive contamination and soft tissue loss.


















































![PERI-PROSTHETIC FRACTURE NAIL-PLATE CONSTRUCT [NPC].pptx](https://cdn.slidesharecdn.com/ss_thumbnails/drarunkumardrmohamedashrafperiprostheticfrasturenail-plateconstructnpc-260209164459-7e9d15a1-thumbnail.jpg?width=640&height=640&fit=bounds)
















