Download to read offline

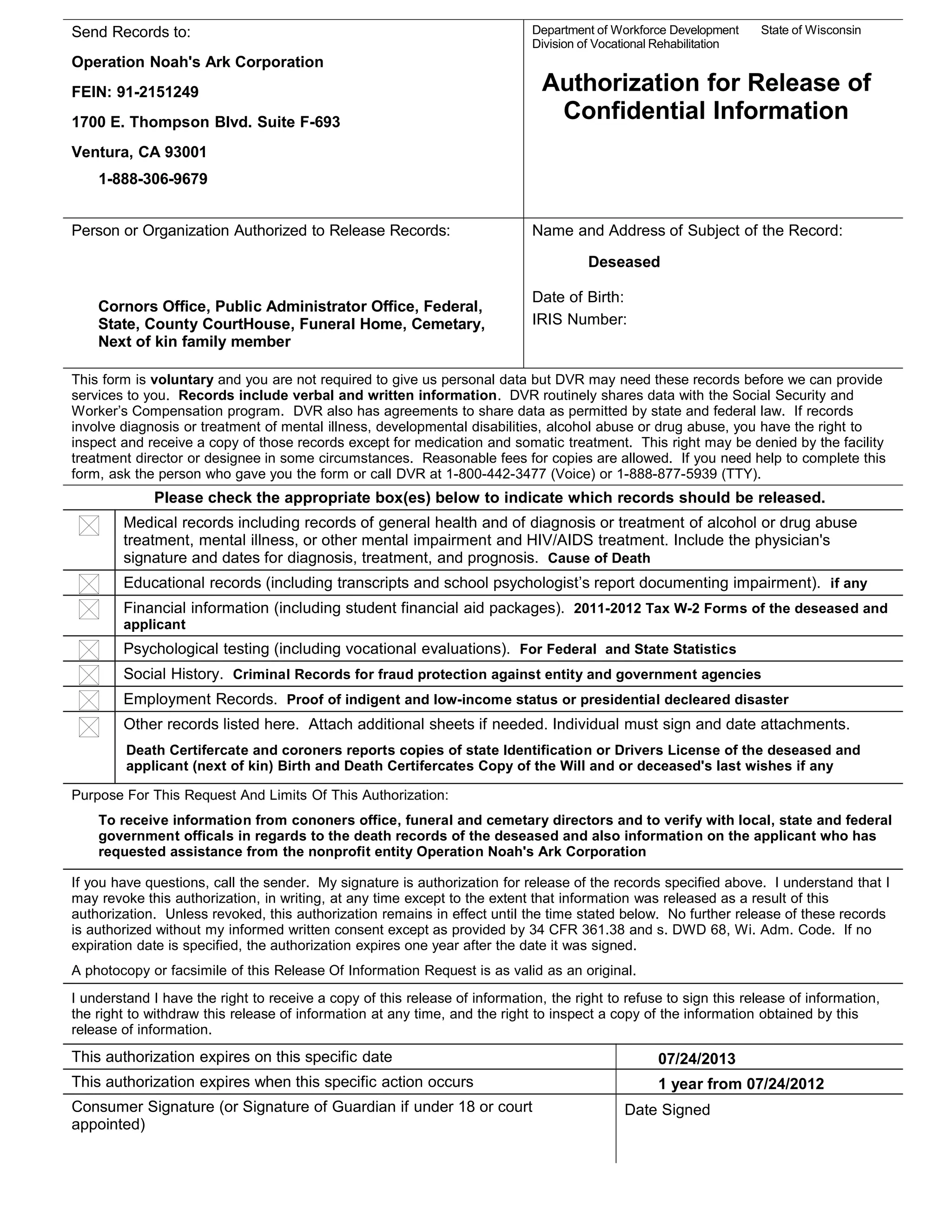


This document authorizes the release of confidential records related to a deceased individual to Operation Noah's Ark Corporation. It allows Noah's Ark to obtain medical, educational, financial, psychological, social, employment, and death records from coroners offices, funeral homes, cemeteries, and government agencies. The purpose is to verify death records and information about the applicant, who is next of kin, in order to provide assistance through Noah's Ark's nonprofit services. The authorization is valid for one year unless an earlier expiration date is specified.






















































![Ercc%20 id%20app 2012[1][1]](https://cdn.slidesharecdn.com/ss_thumbnails/ercc20id20app-201211-120625224840-phpapp01-thumbnail.jpg?width=640&height=640&fit=bounds)


































