Intoduction
Infective endocarditisis an infection of the
endocardial surface of the heart.
may occur as an acute, fulminating infection,
but more commonly runs an insidious course
and is known as subacute bacterial
endocarditis (SBE.)
The annual incidence in the UK is 6-7 per 100
000, but it is more common in developing
countries.
3.
Aetiology
Endocarditis isusually the consequence of two
factors: the presence of organisms in the
bloodstream and abnormal cardiac endothelium
facilitating their adherence and growth.
Factors causing a bacteraemia
Anything that results in a breach of the body's innate
defences can potentially cause a bacteraemia.
4.
factors thatfacilitate the entry of organisms into the
bloodstream.
This may be patient orientated:
poor dental hygiene,
intravenous drug use,
soft tissue infections; or
iatrogenic:
dental treatment,
intravascular cannulae (especially central),
cardiac surgery, or permanent pacemakers.
5.
Local cardiacfactors
Damaged vascular endothelium will promote
platelet and fibrin deposition. It is these small
thrombi that allow organisms to adhere and
grow.
more fibrin and platelets are deposited,
forming the characteristic infected vegetation.
Abnormal vascular endothelium can be the
result of valvular lesions, VSD or a PDA
6.
it ismore common in VSD than ASD, and rare in
MVD without significant regurgitation.
Aortic and mitral valves are the commonest valves to
be affected.
Right-sided endocarditis is typically related to
intravenous drug use
Instrumentation of the right heart (central venous
catheter and temporary pacemaker insertion) is also
a common cause of right-sided endocarditis.
Virulent pathogens such as Staph aureus and Strept
pneumoniae may adhere and multiply on previously
normal valves.
7.
Common organisms andthe sources of
infections
Mouth:
dental disease or procedures a haemolytic viridans
streptococci (Strep, mutans, Strep, sanguis, Strep,
oratis, Strep, milleri) 1/3-1/2 of cases more in
underdeveloped countries
Prolonged indwelling vascular catheters
(especially for TPN)
and antibiotic use and IVDAs who dissolve heroin in
infected lemon juice
Staph. Aureus, Candida (rare)
8.
Gut andperineum:
underlying genitourinary disease or
procedures, or prolonged hospitalization
Enterococci e.g. £. Faecalis (1/5 of cases;
may cause urinary sepsis}
Bowel malignancy
Strep, bovis (rare
9.
Native andprosthetic valve endocarditis:
• Early (poor prognosis): occurring within 60
days of valve surgery and acquired in the
theatre or soon thereafter perhaps on the
intensive care unit
Most commonly caused by: Staph. aureus
and Staph. epidermidis.
10.
Late: occurringmore than 60 days after valve
surgery and presumed to have been acquired in the
community (haematologically spread)
Caused by:
- Strep, viridans (50-70%)
- Staph. aureus (25%)
Soft tissue infections
especially in diabetes and i.v. drug abusers and
patients with long-standing (and poorly cared for) i.v.
catheters: staphylococci
11.
Rare causes
Theseinclude the HACEK group of organisms
(Haemophilus species (H. parainfluenzae, H.
aphrophilus, and H. paraphrophilus, though not H.
influenzae), Actinobacillus actinomycetemcomitans,
Cardiobacterium hominis, Eikenella corrodens, and
Kingella kingae) and tend towards a more insidious
course.
12.
Culture-negative endocarditis
This accounts for 5-10% of endocarditis
cases. The usual cause is prior antibiotic
therapy but some cases are due to a variety
of fastidious organisms that fail to grow in
normal blood cultures.
These include Coxiella bumetii (the cause of
Q fever), Chlamydia spp., Bartonella spp.
(organisms that cause trench fever and cat
scratch disease) and Legionella.
13.
Clinical presentation
Patientscan present with an acute illness and the
classic features of a new or changing heart murmur
and a fever.
they may also present with a subacute insidious
illness. A high index of suspicion for the possibility of
endocarditis is therefore required; otherwise the
diagnosis can easily be delayed.
Clinical signs tend to arise from the following
pathological processes: systemic features of
infection; cardiac lesions; embolization, and immune
complex deposition
Clinical presentation
Distalembolization may result in infarction of
the distal organ, and/ or spread of infection.
The signs and symptoms will depend on the
organ involved.
cerebral abscess can present with seizures,
loss of consciousness or focal neurological
signs.
Clubbing occurs in 10%.
18.
Diagnostic criteria
Criteriafor the diagnosis of infective endocarditis is
known as the Duke criteria
Duke criteria for the diagnosis of infective
endocarditis (IE)
A diagnosis of IE can be made if
two major criteria,
one major and three minor, or
five minor criteria are present.
19.
Major criteria
Positive blood culture for infective
endocarditis
Expected microorganisms for infective
endocarditis from two separate blood
cultures - viridans streptococci,* HACEK*
groups, Streptococcus bovis, or
community-acquired Staphylococcus
aureus or enterococci, without known
primary focus, or M
20.
Persistently positiveblood culture,
defined as growth and identification of a
microorganism consistent with IE
originating from:
- blood cultures that are obtained
more than 12 hours apart, or
3/3 or 3/4 or more separate blood
cultures, with the first and last blood
cultures obtained at least 60 minutes
apart
21.
Evidence ofendocardial involvement
supporting the diagnosis of IE
Echocardiogram findings
(a) Oscillating intracardiac mass present:
- on valve or supporting structures, or
- in the path of regurgitant bloodstream
flow, or
- on implanted material, in the absence of
an alternative anatomical explanation, or
22.
(b) Abscess, or
(c)Newly identified partial
dehiscence of prosthetic
valve, or New valvular
regurgitation
23.
Minor criteria
Fever: = or > 38°C (100.4°F)
Predisposition to IE: heart condition predisposing to
IE, or intravenous drug abuse (IVDA)
Echocardiogram: findings may be consistent with IE,
but major criteria as stated above are not met
Immunological phenomena present: Roth
spots,Osler's nodes, glomerulonephritis, rheumatoid
factor via laboratory analysis
24.
Microbiological evidenceof IE: blood cultures are
positive but major criteria are not met as previously
described,* or
serological studies support an infection that is
consistent with the diagnosis of IE
Vascular phenomena present: major arterial emboli,
mycotic aneurysm, septic pulmonary infarcts,
conjunctival haemorrhages, intracranial
haemorrhage, Janeway lesions
25.
Investigations
The purposeis threefold:
confirm the diagnosis of infective
endocarditis;
to identify the causative organism to
ensure appropriate therapy;
to monitor the patient's response to
therapy.
26.
Blood culturesare the key diagnostic
investigation in infective endocarditis.
At least three sets of samples (i.e six
bottles) should be taken and there
should be liaison with the microbiology
department. The yield of any test is
increased by the amount of information
about the subject given
27.
Serological testscan be sent when the
diagnosis is suspected and the blood cultures
are negative.
They aid diagnosis in cases where the
organisms will not grow in standard blood
cultures (i.e. Coxiella, Bartonella, Legionella
and Chlamydia).
28.
Other laboratory tests
Full blood count. A normochromic normocytic
anaemia and polymorphonuclear leucocytosis are
common. Thrombocytopenia or thrombocytosis can
occur.
Urea and electrolytes. Renal dysfunction is a
complication of sepsis. Electrolyte disturbance should
be identified and corrected primarily in any patient
prone to arrhythmias.
Liver biochemistry is often mildly deranged with, in
particular, an increased serum alkaline phosphatase.
29.
Inflammatory markers.C-reactive protein and
erythrocyte sedimentation rate are non-specific
markers of inflammation and are increased in any
infection. CRP tends to respond more acutely than
ESR.
Immunoglobulins and complement. Serum
immunoglobulins are increased, but total complement
and C3 complement are decreased owing to immune
complex formation.
30.
Urine. Proteinuriamay occur and microscopic
haematuria is nearly always present.
Polymerase chain reaction (PCR) is used to
recover specific DNA or RNA from blood,
urine, or surgically excised tissue.
31.
Electrocardiogram
This mayshow evidence of myocardial
infarction (emboli) or conduction defects. New
atrioventricular block is suggestive of abscess
formation.
Patients with suspected IE therefore should
have an ECG on presentation and repeated
regularly during their admission depending on
their clinical course.
32.
Chest X-ray
Thismay show evidence of heart failure or, in
right-sided endocarditis, multiple pulmonary
emboli and/or abscesses.
The combination of sepsis and pulmonary
infiltrates on chest X-ray should alert the
clinician to the possibility of right-sided
endocarditis.
33.
Echocardiography
Transthoracic echocardiography(TTE) is rapid, non-
invasive and has high specificity for visualizing
vegetations although sensitivity is 60-75%. It is also
useful in documenting valvular dysfunction and other
local complications, such as aortic root abscesses.
Transoesophageal echocardiography (TOE) has a
higher sensitivity and specificity for abscess
formation because of the close physical proximity of
the transducer to the aortic root. TOE also enhances
the visualization of prosthetic valves and is
recommended for all cases of suspected prosthetic
valve endocarditis.
34.
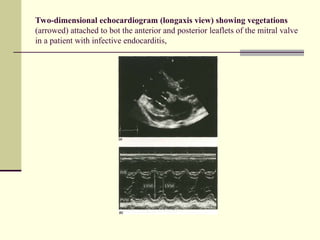
Two-dimensional echocardiogram (longaxisview) showing vegetations
(arrowed) attached to bot the anterior and posterior leaflets of the mitral valve
in a patient with infective endocarditis,
35.
Principles of therapy
Therapy of endocarditis is difficult because
organisms reside within a protected site
within the vegetation.
High concentrations of intravenous antibiotic
are required for prolonged periods to achieve
successful treatment.
synergistic combinations of antibiotics are
used, in order to maximize the microbiocidal
effect.
36.
This isbest achieved by a multidisciplinary approach
consisting of clinicians, cardiologists, cardiothoracic
surgeons and microbiologists.
Drug therapy
Empirical antibiotic treatment is started only after
cultures are taken. The regimen is then adjusted
according according to culture results.
The treatment should continue for 4-6 weeks,
although studies of 2-week.
37.
Serum levelsof gentamicin and vancomycin
need to be monitored.
In patients with penicillin allergy one of the
glycopeptide antibiotics, vancomycin or
teicoplanin, can be used.
Penicillins, however, are fundamental to the
therapy of bacterial endocarditis; allergies
therefore seriously compromise the choice of
antibiotics.
38.
Persistent fever
Mostpatients with infective endocarditis
should respond within 48 hours of initiation of
appropriate antibiotic therapy.
This is evidenced by a resolution of fever,
reduction in serum markers of infection (CRP
tends to be the most sensitive) and relief of
systemic symptoms of infection.
39.
Failure ofthis to occur needs to be taken very
seriously. The following should be considered:
perivalvular extension of infection and possible
abscess formation
drug reaction (the fever should promptly resolve after
drug withdrawal)
nosocomial infection (i.e. venous access site, UTI)
pulmonary embolism (as a consequence of right-
sided endocarditis or prolonged hospitalization).
40.
In suchcases, samples for culture should be taken
from all possible sites and evidence sought for the
above causes.
Changing antibiotic dosage or regimen should be
avoided unless there are positive cultures or a drug
reaction is suspected.
Emergence of bacterial resistance is uncommon.
Close liaison with microbiology is recommended and
a cardiothoracic surgical opinion should be sought.
41.
Surgery
Surgical interventionshould be considered in
the following cases:
extensive damage to a valve
prosthetic valve endocarditis (valve
replacement is usually required)
persistent infection despite therapy
large vegetations
serious embolization
42.
myocardial abscess
fungal endocarditis (this is usually refractory to
antimicrobial therapy)
progressive cardiac failure.
Early liaison with a cardiothoracic surgeon is
essential. It
is desirable to eradicate active infection before any
surgical intervention, but if antibiotic therapy is failing,
with progressive cardiac failure, uncontrolled sepsis
or severe emboli, it will not be possible to wait. In
general, early surgery is preferable.
43.
Prevention
Control andprevention of RF will prevent rheumatic
heart disease and thus associated endocarditis.
People with valvular lesions who are at moderate to
high risk of developing endocarditis are
recommended to receive antibiotic therapy before
undergoing a procedure likely to result in a
bacteraemia, such as dental treatment, endoscopy or
surgical instrumentation.
There are no randomized placebo-controlled trials to
assess the efficacy of such antibiotic prophylaxis, and
hence its value has been questioned. It is argued that
with uncertain benefits, there is a greater risk of an
anaphylactic reaction from widespread penicillin use.
44.
Meticulous oraland skin hygiene is also significant in
preventing endocarditis.
Many cases of hospital-acquired endocarditis can be
prevented by better care during insertion and
handling of intravascular catheters, and
prompt removal if they become infected.
recommend the selected use of antibiotic
prophylaxis, e.g. with prosthetic valves in those
patients who are at a significantly increased risk of
developing endocarditis whilst undergoing certain
procedures known to cause a bacteraemia.
















![Infective Endocarditis Group [A7] Seminar](https://cdn.slidesharecdn.com/ss_thumbnails/infectiveendocarditisa7-250627114414-bb3356a5-thumbnail.jpg?width=640&height=640&fit=bounds)

























![ONFH[AVN HIP] -TRIPLE REGIME -A NOVAL SURGICAL CONCEPT .pptx](https://cdn.slidesharecdn.com/ss_thumbnails/onfhavnhip2026koaconcalicutdrgokuldevdrmashraf-260210064517-213ec005-thumbnail.jpg?width=640&height=640&fit=bounds)






