2
CONTENTS
• Introduction
• Definitions
•History of Complete Dentures
• Theories of Impression Making
• Principles of Impression Making
• Objectives of Impression Making
• Conclusion
• References
3.
3
INTRODUCTION
Impression generallyis a negative likeness or copy in reverse of the
surface of an object.
Dental Impression: A negative imprint of an oral structure used to
produce a positive replica of the structure to be used as a permanent
record or in the production of a dental restoration or prosthesis.
The beginning of a good denture starts with making of a good
impression, so a good impression is a stepping stone.
4.
4
DEFENITION
Complete dentureis defined as a removable dental prosthesis that replaces the
entire dentition and associated structures of the maxillae or mandible.
5.
5
HISTORY
• 1711 MatthianG. Purman introduced the use of wax.
• 1844 Plaster of paris was first used as an impression material.
• 1845-1899 concepts of atmospheric pressure, maximum extension of
denture bearing area,equal distribution of pressure and close
adaptation of the denture bearing tissues were stressed.
• 1928 Pierre Fauchard made dentures by measuring the mouth with
compasses and cutting bone into an approximate shape.
6.
6
• 1951 Car/ O Boucher introduced selective pressure theory..
• 1896 Green brother introdued mucocompressive theory.
• 1900-1929 Concepts like Rebase impressions, border molding and
techniques for flabby tissues were introduced.
• 1930-1940 This era recognized the anatomy of the denture bearing
areas, and muscle physiology as related to impression procedures. This
is evident by descriptions of border molding of dentures.
7.
7
several new impressionmaterials were introduced : reversible
hydrocolloids, zinc oxide eugenol and zinc oxide and oil of cloves.
• 1950-1964 more emphasis on biologic factor of impression making was
given.
• 1965-1980 new techniques to manage compromised situations were
introduced
• New techniques are periodically been formulated to overcome the
drawbacks faced.
8.
Prosthetic treatment foredentulous patients, Zarb, Bolender, 12th edition , Syllabus of Complete denture, Charles M.
Heartwell, 4th edition
8
THEORIES OF IMPRESSION MAKING
• Most of the impressions of the twentieth century are made with a view to
functional movement of the musculature.
• Theoretically, the impressions are so formed that the complete denture
will require no change in contour. This happens often with upper
dentures but no so often with lower dentures.
9.
Prosthetic treatment foredentulous patients, Zarb, Bolender, 12th edition , Syllabus of Complete denture, Charles M.
Heartwell, 4th edition
9
Impression are made with:
Definitive pressure impressions
Minimal pressure impressions
Selective-pressure impressions
Functional impression technique
10.
Prosthetic treatment foredentulous patients, Zarb, Bolender, 12th edition , Syllabus of Complete denture, Charles M.
Heartwell, 4th edition
10
DEFINITIVE PRESSURE IMPRESSION
Because denture retention is tested most severely during
mastication, many dentist formerly considered it essential for the tissue to
remain in contact with the denture during chewing.
However; dentures did not fit well at rest, because of
» Tissue so distorted, tend to rebound.
» Tissues so abused will long maintain the shape that they assumed on
the day of impression.
11.
Prosthetic treatment foredentulous patients, Zarb, Bolender, 12th edition , Syllabus of Complete denture, Charles M.
Heartwell, 4th edition
11
Many of the proponents of this group advocates the use of closed mouth
techniques.
Aside the disadvantages of pressure impression technique mentioned above,
the closed mouth technique do not allow adequate muscle trimming of the
periphery.
Very often dentures made with this technique are over-extended and must be
arbitrarily trimmed.
12.
Prosthetic treatment foredentulous patients, Zarb, Bolender, 12th edition , Syllabus of Complete denture, Charles M.
Heartwell, 4th edition
12
Advocates were not always able to actually obtain the desired pressure but
tended to create excessive pressure.
Dentures often resulted in good initial retention but eventually bone
resorption and loose dentures.
13.
Prosthetic treatment foredentulous patients, Zarb, Bolender, 12th edition , Syllabus of Complete denture, Charles M.
Heartwell, 4th edition
13
MINIMAL PRESSURE IMPRESSIONS
The popularization of this techniques is in the early forties.
Idea was not new, however for Richardson in 1896 had advocated plaster
because it least disturbed the tissues.
Addison in 1994, descirbed the so called "mucostatic impression" and
attributed to page. This was based on theories and were not applicable in
the oral cavity.
14.
Prosthetic treatment foredentulous patients, Zarb, Bolender, 12th edition , Syllabus of Complete denture, Charles M.
Heartwell, 4th edition
14
Main point of the mucostatic principle concerned pascal's law, which
states that pressure on a confined liquid, will be transmitted throughout
the liquid in all directions.
According to this concept, the mucosa, being more than 80 % water, will
react like liquid in a closed vessel and thus cannot be compressed.
This is not true, as tissue fluids can easily escape under the border of a
denture. Hence mucosa is not a closed vessel.
15.
Prosthetic treatment foredentulous patients, Zarb, Bolender, 12th edition , Syllabus of Complete denture, Charles M.
Heartwell, 4th edition
15
According to principle of mucostatics, impression material should
record, without distortion every detail of the mucosa so that complete
denture would fit all minute elevations and depressions.
So much emphasis on recording detail was placed that even seperating
medium could not be used at any point in the procedure.
Mucostatics further demanded that a metal base be used rather than the
dimensionally unstable acrylic.
16.
Prosthetic treatment foredentulous patients, Zarb, Bolender, 12th edition , Syllabus of Complete denture, Charles M.
Heartwell, 4th edition
16
Gold, one Of the most accurate metals, was by passed in favor of a
chrome alloy. Thus another minor inaccuracy was added.
Mucostatics further demanded that a metal base be used rather than the
dimensionally unstable acrylic.
Most Important of all, mucosal typography, is not static over a 24-hour
period.
17.
Prosthetic treatment foredentulous patients, Zarb, Bolender, 12th edition , Syllabus of Complete denture, Charles M.
Heartwell, 4th edition
17
There is difference between the mucosal contours just after rising in the
morning, and that which exists after 12 hours in the upright position.
(Stephens et al, 1966)
So all the infinite details achieved in the impression would be altered by
the time the denture is finished.
The adherents of the mucostatic principle considered interfacial surface
tension as the only important retentive mechanism in complete dentures.
18.
Prosthetic treatment foredentulous patients, Zarb, Bolender, 12th edition , Syllabus of Complete denture, Charles M.
Heartwell, 4th edition
18
SELECTIVE PRESSURE TECHNIQUE
This principle is based on the belief that the mucosa over the ridge is best
able to withstand pressure, whereas that covering the midline is thin and
contains very little submucosal tissues. (Boucher, 1951).
Boucher advocated that this technique combines the principles of both
pressure and non pressure procedures.
The technique utilizes a preliminary compound impression that is
generously relieved over the midline and incisive papilla areas.
19.
Prosthetic treatment foredentulous patients, Zarb, Bolender, 12th edition , Syllabus of Complete denture, Charles M.
Heartwell, 4th edition
19
The final impression is taken in plaster, which acts as a wash and also
records the relieved areas with minimal pressure while the ridge areas are
undergoing considerable pressure.
Thus, the midline and papilla sections of the denture will not make contact
with the mucosa when the denture is not in function, but by the same token,
they will not bear heavily when the patient is chewing.
20.
Prosthetic treatment foredentulous patients, Zarb, Bolender, 12th edition , Syllabus of Complete denture, Charles M.
Heartwell, 4th edition
20
Points to keep in mind:
Most fine denture are made with this principle.
This technique demands firm , healthy mucosal covering over the ridge.
If flabby ridge exist , it is preferable to use a minimal pressure impression.
This technique optimizes the stability and retention of the prosthesis
21.
Prosthetic treatment foredentulous patients, Zarb, Bolender, 12th edition , Syllabus of Complete denture, Charles M.
Heartwell, 4th edition
21
FUNCTIONAL IMPRESSION TECHNIQUE
This technique uses a complete denture that is delivered, relieved on its
internal aspects, and filled with a slow setting impression material(tissue
conditioning material).
The patient wears the prosthesis for several days, allowing the tissues to be
recorded ‘’in function’’.
The completed impression then is converted to and reline material via
laboratory processing.
22.
Prosthetic treatment foredentulous patients, Zarb, Bolender, 12th edition , Syllabus of Complete denture, Charles M.
Heartwell, 4th edition
22
This technique seeks to create a denture base that models the functionally
loaded tissues.
23.
Prosthetic treatment foredentulous patients, Zarb, Bolender, 12th edition , Syllabus of Complete denture, Charles M.
Heartwell, 4th edition
23
PRINCIPLES OF IMPRESSION MAKING
• The concepts to be followed to get successful impression are:-
The oral tissues must be healthy.
Impression should include all of the basal seat within the limits of
health and function of the supporting and limiting tissues.
The borders must be in harmony with the anatomical and
physiological limitation of the oral structures.
Physiological type of border moulding should be performed.
24.
Prosthetic treatment foredentulous patients, Zarb, Bolender, 12th edition , Syllabus of Complete denture, Charles M.
Heartwell, 4th edition
24
Sufficient space should be provided within the impression tray for the
selected impression material.
Impression must be removed from the mouth without damaging the
mucosa.
Selective pressure should be applied on the basal seat during impression
making.
A guiding mechanism should be provided for correct positioning of the
tray within the mouth.
25.
Prosthetic treatment foredentulous patients, Zarb, Bolender, 12th edition , Syllabus of Complete denture, Charles M.
Heartwell, 4th edition
25
The tray and impression material should be made of dimensionally stable
materials.
The external shape of the impression should be similar to the external
form of complete denture.
26.
Prosthetic treatment foredentulous patients, Zarb, Bolender, 12th edition , Syllabus of Complete denture, Charles M.
Heartwell, 4th edition
26
OBJECTIVES OF IMPRESSION MAKING
In an impression technique for complete denture , the procedure must
strive for five primary objectives. The objectives are:
Preservation
Support
Retention
Stability
Esthetics
27.
Prosthetic treatment foredentulous patients, Zarb, Bolender, 12th edition , Syllabus of Complete denture, Charles M.
Heartwell, 4th edition
27
PRESERVATION
M.M.De Van’s dictum “It is more important to preserve what already exists
than to replace what is missing” has never been challenged or disapproved.
Preservation of the remaining residual ridges is one objective.
It is physiologically accepted that with the loss of stimulation of the
natural teeth the alveolar ridge will atrophy or resorb. This process varies
in individual.
28.
Prosthetic treatment foredentulous patients, Zarb, Bolender, 12th edition , Syllabus of Complete denture, Charles M.
Heartwell, 4th edition
28
This process can be hastened or retarded by local factors.
Pressure in the impression technique is reflected as pressure in the
denture base and results in soft tissue damage and bone resorption.
29.
Prosthetic treatment foredentulous patients, Zarb, Bolender, 12th edition , Syllabus of Complete denture, Charles M.
Heartwell, 4th edition
29
Hence, in impression making, this rule is followed by not using heavy
pressure and by not covering as much of the supporting areas as possible to
minimize the possibility of the soft tissue abuse and bone resorption.
Other factors such as
• Occlusion
• Interocclusal distance
• Centric relation in harmony with centric occlusion are of great importance.
30.
Prosthetic treatment foredentulous patients, Zarb, Bolender, 12th edition , Syllabus of Complete denture, Charles M.
Heartwell, 4th edition
30
SUPPORT
Denture support is the resistance to vertical forces of mastication and to
occlusal or other forces applied in a direction towards the basal seat.
When the natural teeth are missing , the alveolar ridge and their coverage of
mucosal tissues becomes the supporting elements.
They were never meant to endure the forces of mastication and other constant
occlusal pressures that result from swallowing, clenching and bruxing.
31.
Prosthetic treatment foredentulous patients, Zarb, Bolender, 12th edition , Syllabus of Complete denture, Charles M.
Heartwell, 4th edition
31
To make the best of a bad situation, it is necessary to enhance the available
support by utilizing maximum coverage of all usable ridge bearing areas.
Must be accomplished without interference of routine movements or
function of the stomatognathic system.
32.
Prosthetic treatment foredentulous patients, Zarb, Bolender, 12th edition , Syllabus of Complete denture, Charles M.
Heartwell, 4th edition
32
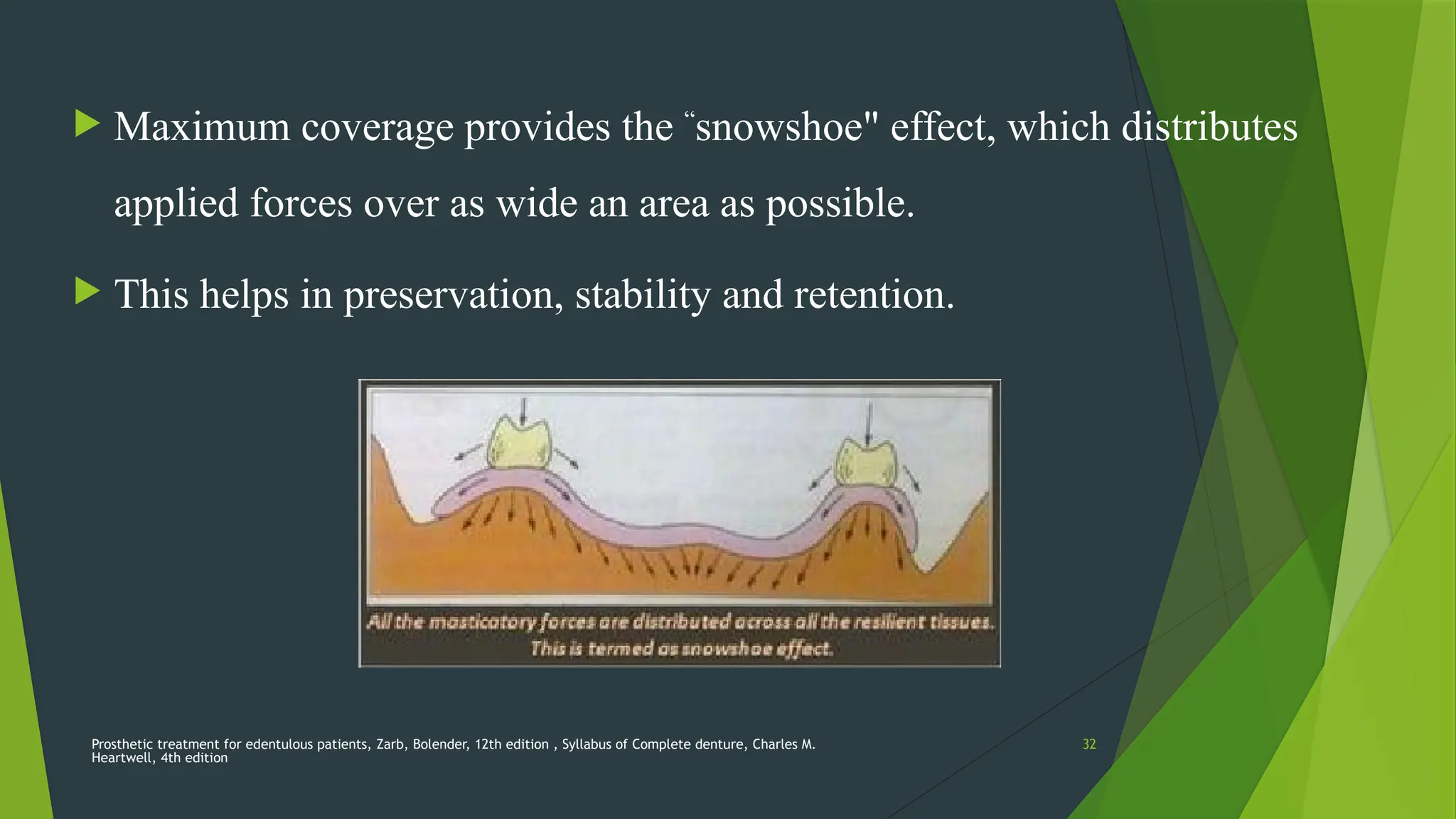
Maximum coverage provides the “
snowshoe" effect, which distributes
applied forces over as wide an area as possible.
This helps in preservation, stability and retention.
33.
Prosthetic treatment foredentulous patients, Zarb, Bolender, 12th edition , Syllabus of Complete denture, Charles M.
Heartwell, 4th edition
33
Areas of support
Divided into:
1. Primary
2. Secondary
3. Slight
1. Primary support
• Areas of edentulous ridge that are at right angles to occlusal forces do
not resorb easily.
34.
Prosthetic treatment foredentulous patients, Zarb, Bolender, 12th edition , Syllabus of Complete denture, Charles M.
Heartwell, 4th edition
34
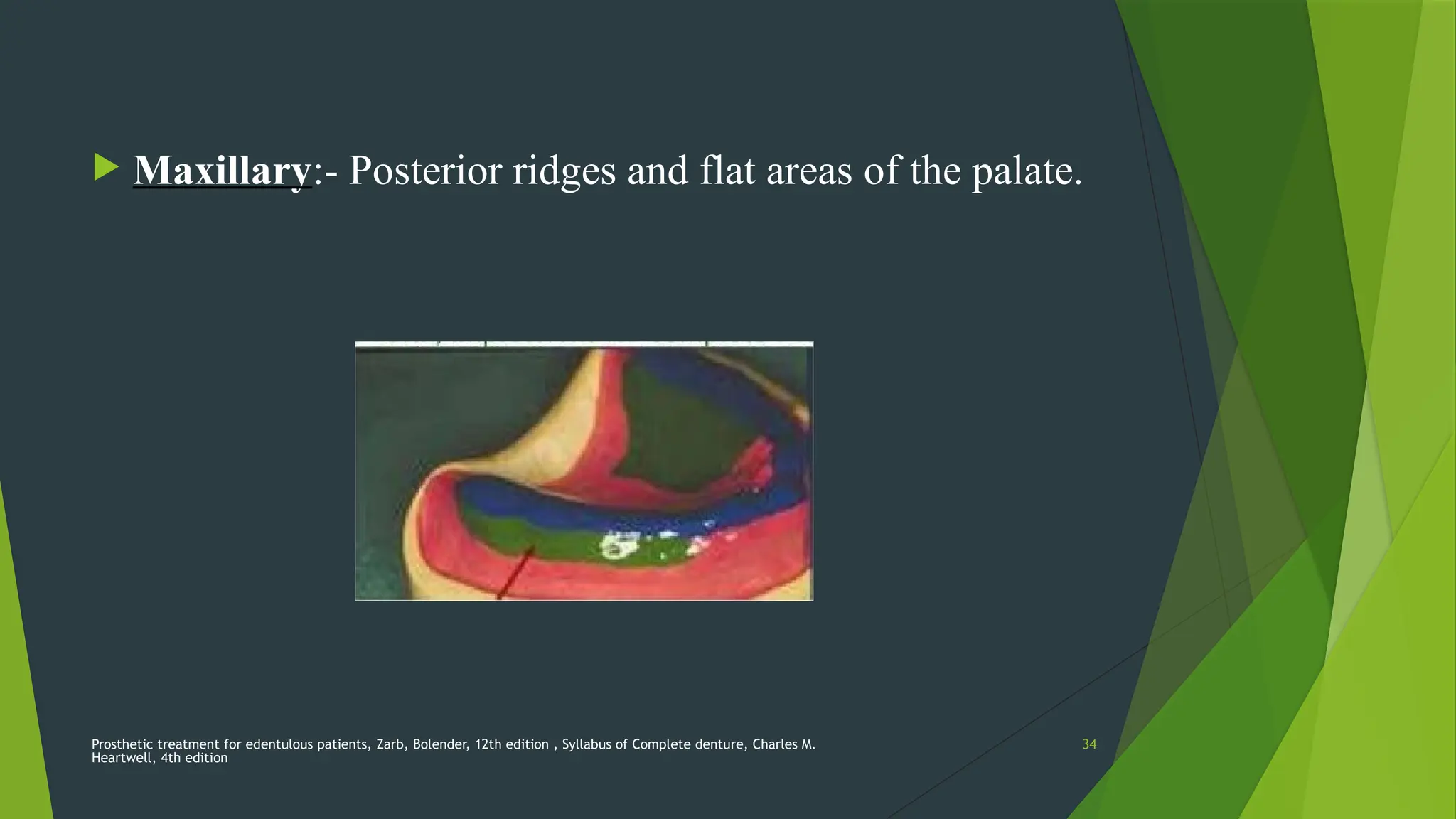
Maxillary:- Posterior ridges and flat areas of the palate.
35.
Prosthetic treatment foredentulous patients, Zarb, Bolender, 12th edition , Syllabus of Complete denture, Charles M.
Heartwell, 4th edition
35
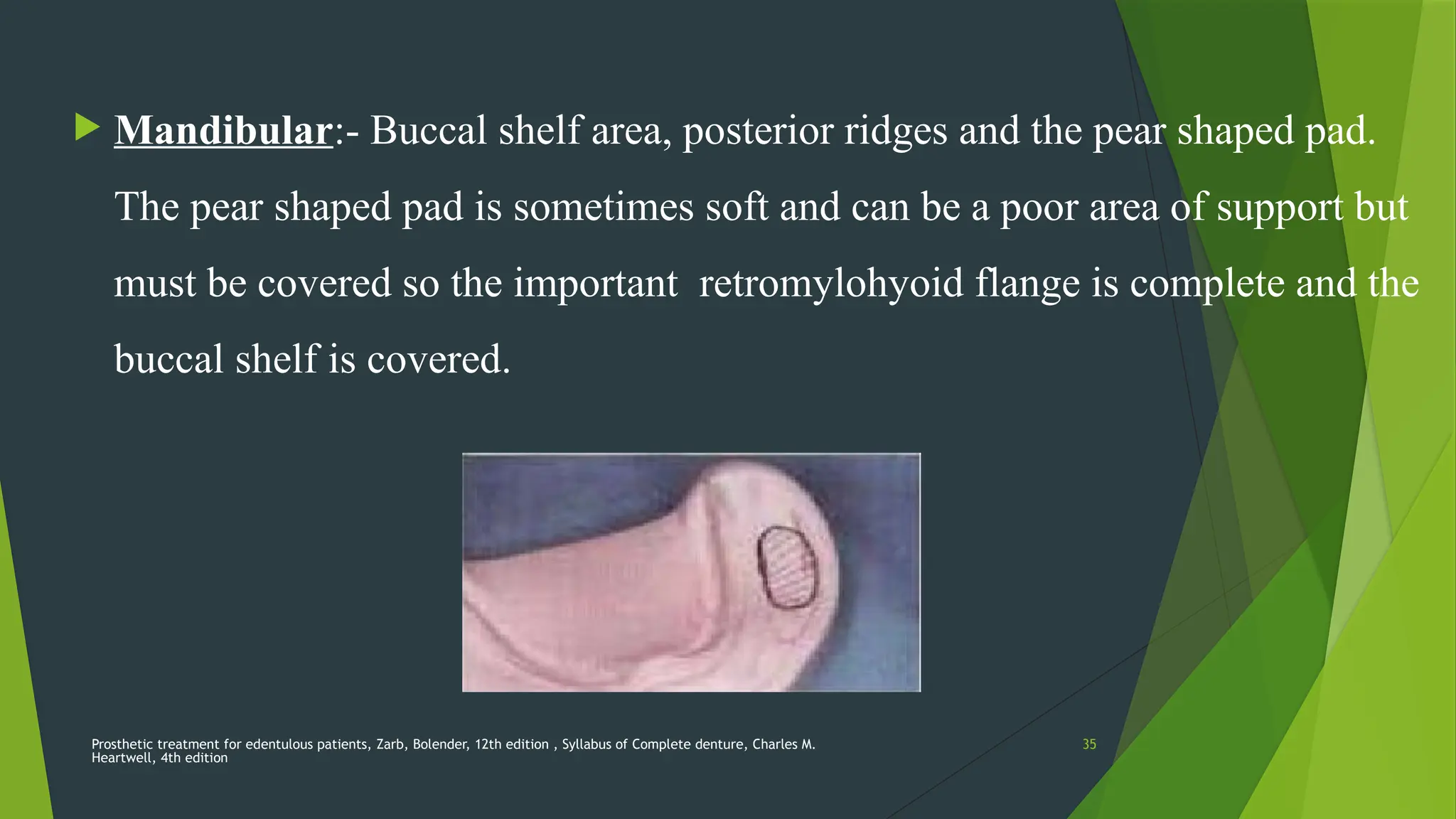
Mandibular:- Buccal shelf area, posterior ridges and the pear shaped pad.
The pear shaped pad is sometimes soft and can be a poor area of support but
must be covered so the important retromylohyoid flange is complete and the
buccal shelf is covered.
36.
Prosthetic treatment foredentulous patients, Zarb, Bolender, 12th edition , Syllabus of Complete denture, Charles M.
Heartwell, 4th edition
36
2. Secondary support
• Areas of the edentulous ridge that are greater than at right angles to
occlusal forces or are parallel to them; also the areas of the
edentulous ridge that are at right angles to occlusal forces tend to
resorb under load.
• For example, the anterior ridge is known to resorb at a much faster
rate than the posterior ridge areas where it is subjected to load.
37.
Prosthetic treatment foredentulous patients, Zarb, Bolender, 12th edition , Syllabus of Complete denture, Charles M.
Heartwell, 4th edition
37
• Maxillary :- Anterior ridge and all ridge slopes
• Mandibular :- Anterior ridge and all ridge slopes
3. Slight
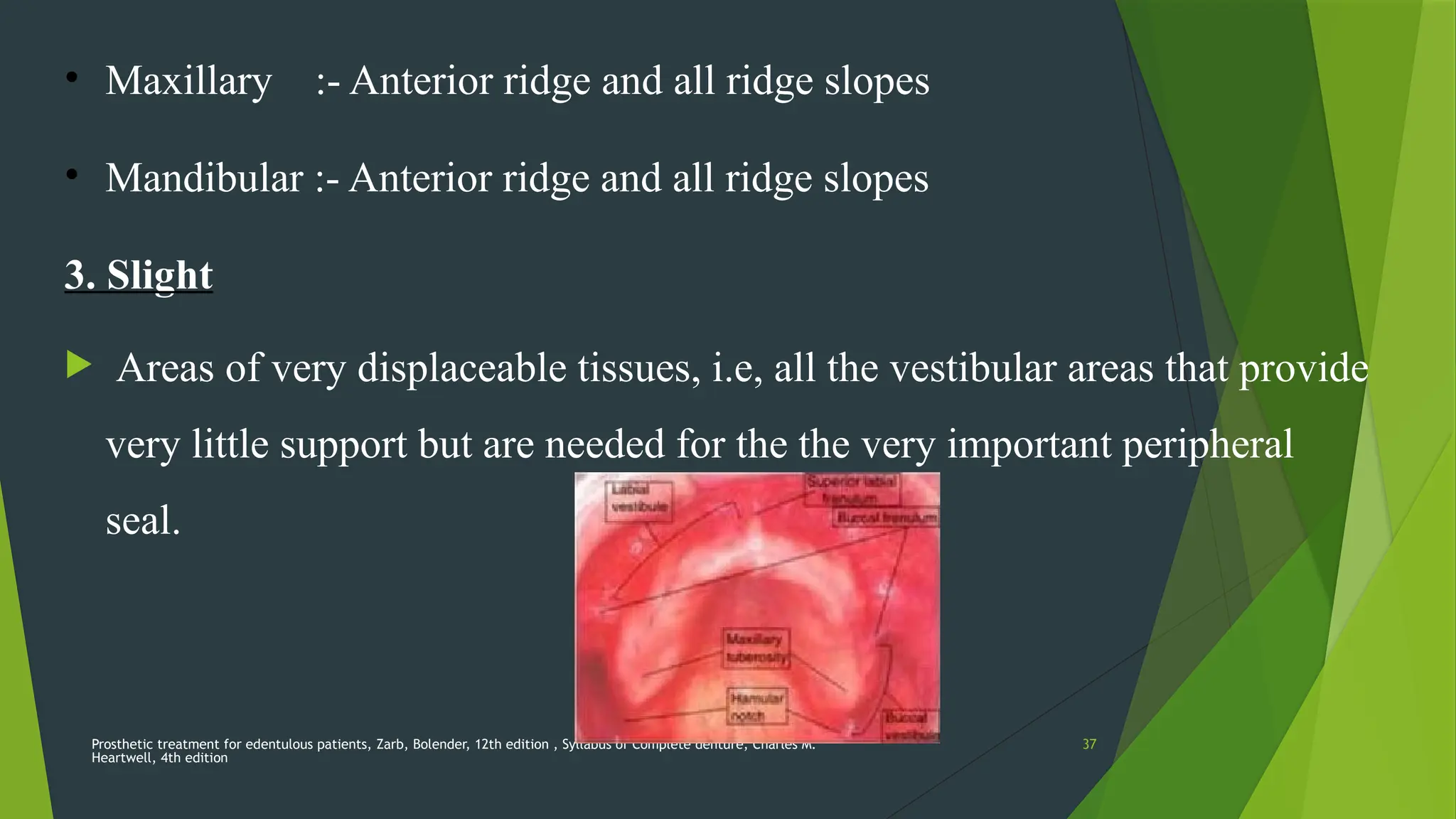
Areas of very displaceable tissues, i.e, all the vestibular areas that provide
very little support but are needed for the the very important peripheral
seal.
38.
Prosthetic treatment foredentulous patients, Zarb, Bolender, 12th edition , Syllabus of Complete denture, Charles M.
Heartwell, 4th edition
38
Importance of covering the Buccal shelf
Buccal shelf is the area of bone between the extraction sites of the molars
and the external oblique line. The cortical plate over the site of the extracted
teeth is rarely intact and is usually spiculated and rough.
It is intact cortical plate and tends not to resorb due to stimulation of the
attachment of the buccinator muscle.
39.
Prosthetic treatment foredentulous patients, Zarb, Bolender, 12th edition , Syllabus of Complete denture, Charles M.
Heartwell, 4th edition
39
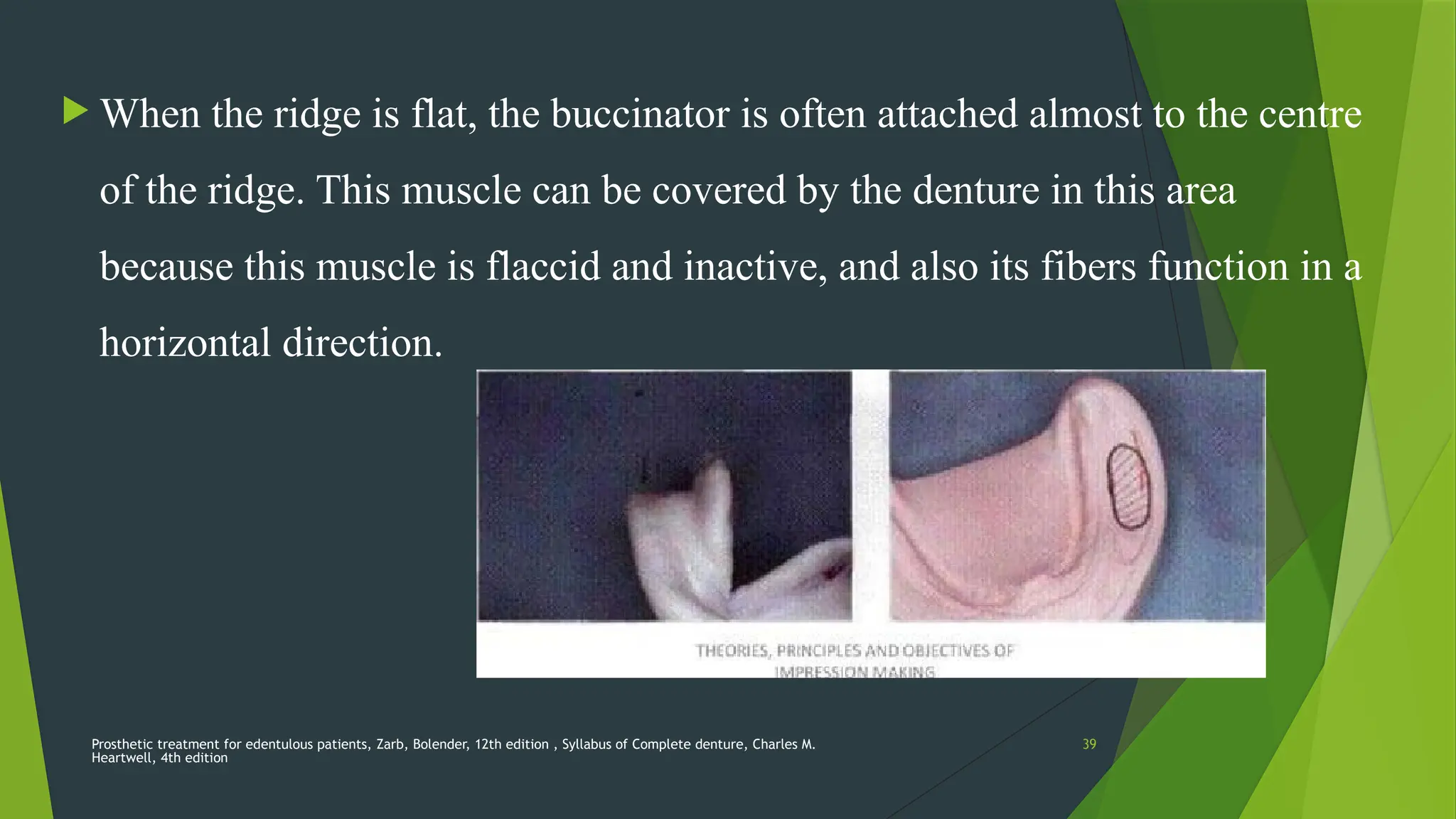
When the ridge is flat, the buccinator is often attached almost to the centre
of the ridge. This muscle can be covered by the denture in this area
because this muscle is flaccid and inactive, and also its fibers function in a
horizontal direction.
40.
Prosthetic treatment foredentulous patients, Zarb, Bolender, 12th edition , Syllabus of Complete denture, Charles M.
Heartwell, 4th edition
40
Fortunately, in rare old patients, buccinator is tense and active, then it is
more difficult to cover buccal shelf area (tend to have flatter ridges).
i.e., thin spiney, or flat, the buccal shelf is usually the only available area
of support.
41.
Prosthetic treatment foredentulous patients, Zarb, Bolender, 12th edition , Syllabus of Complete denture, Charles M.
Heartwell, 4th edition
41
Importance of covering the retromolar pad
The reason the pear-shaped pads so important is that it is an area that
rarely resorbs.
Because the very large and active temporalis muscle inserts on the
coronoid process and also on the anterior border of the ramus with the
tendons ending on the alveolar bone distal to the pad.
Important to include the pad in the impression so that it can be used as
a land mark for the placement of the occlusal plane.
42.
Prosthetic treatment foredentulous patients, Zarb, Bolender, 12th edition , Syllabus of Complete denture, Charles M.
Heartwell, 4th edition
42
Bone responds to tensile stimulation by growth and apposition, which
causes areas of muscle attachments not to resorbs .
Eg: Genial tubercle and mylohyoid ridges
Pad is on an area of bone that is relatively stable
43.
Prosthetic treatment foredentulous patients, Zarb, Bolender, 12th edition , Syllabus of Complete denture, Charles M.
Heartwell, 4th edition
43
Improving Support
There are four basic Methods:-
Surgical removal of pendulous tissue.
Use of tissue-conditioning materials.
Surgical reduction of sharp or spiney mandibular ridge.
Implants
44.
Prosthetic treatment foredentulous patients, Zarb, Bolender, 12th edition , Syllabus of Complete denture, Charles M.
Heartwell, 4th edition
44
RETENTION
Retention of a denture is its resistance to removal in a direction
opposite to that of its insertion.
Retention resist the adhesiveness of foods, the force of gravity, and the
forces associated with the opening of the jaws.
45.
Prosthetic treatment foredentulous patients, Zarb, Bolender, 12th edition , Syllabus of Complete denture, Charles M.
Heartwell, 4th edition
45
Factors involved in the retention of dentures:
• Interfacial force
• Adhesion
• Cohesion
• Oral and facial musculature
• Atmospheric pressure Adhesion,
• Rotation insertion paths and Parallel walls
• Gravity
46.
Prosthetic treatment foredentulous patients, Zarb, Bolender, 12th edition , Syllabus of Complete denture, Charles M.
Heartwell, 4th edition
46
Interfacial forces
"The tension or resistance to separation possed by the film of liquid
between two well-adapted surfaces" - GPT
For better understanding, it is divided into:-
• Interfacial surface tension
• Interfacial viscous tension
47.
Prosthetic treatment foredentulous patients, Zarb, Bolender, 12th edition , Syllabus of Complete denture, Charles M.
Heartwell, 4th edition
47
Interfacial Surface Tension
— It results from a thin layer of fluid that is present between two parallel
planes of rigid material.
— It dependent on the ability of fluid to wet the rigid surrounding material.
48.
Prosthetic treatment foredentulous patients, Zarb, Bolender, 12th edition , Syllabus of Complete denture, Charles M.
Heartwell, 4th edition
48
If the surrounding material has a low surface tension, as oral mucosa does,
fluid will maximize its contact with the material, thereby wetting it readily
and spreading it out in a thin film.
Denture base material vary in their surface tension( termed as wettability),
with processed materials displaying greater wettability than autocured
resins.
49.
Prosthetic treatment foredentulous patients, Zarb, Bolender, 12th edition , Syllabus of Complete denture, Charles M.
Heartwell, 4th edition
49
All the denture base materials have higher surface tension than oral
mucosa, but once by salivary pellicle, their surface tension is reduced,
which promotes maximizing the surface area between liquid and base.
Thus the thin film furnishes retentive force by virtue of the tendency
of the fluid to maximize its contact with both surfaces.
50.
Prosthetic treatment foredentulous patients, Zarb, Bolender, 12th edition , Syllabus of Complete denture, Charles M.
Heartwell, 4th edition
50
Interfacial Viscous Tension
It refers to the force holding two parallel plates together that is due to the
viscosity of the interposed liquid.
It is explained by Stefan's Law.
51.
Prosthetic treatment foredentulous patients, Zarb, Bolender, 12th edition , Syllabus of Complete denture, Charles M.
Heartwell, 4th edition
51
F decreases with the increase in (h )width of the space between the
denture base and the mucosa.
A slow and steady increase in V (velocity of the displacing force) will
have least resistance from interfacial surface tension than a rapid V.
52.
Prosthetic treatment foredentulous patients, Zarb, Bolender, 12th edition , Syllabus of Complete denture, Charles M.
Heartwell, 4th edition
52
To obtain maximum interfacial surface tension:
Saliva should be thin and even.
Denture base should cover a large area.
There should be a good adhesive and cohesive forces, which aid to enhance
interfacial surface tension
53.
Prosthetic treatment foredentulous patients, Zarb, Bolender, 12th edition , Syllabus of Complete denture, Charles M.
Heartwell, 4th edition
53
Adhesion
The physical attraction of unlike molecules to one another" — GPT
Saliva plays an important role in adhesion.
The amount of adhesion present is directly proportional to the denture
base area.
In patients with Xerostomia, adhesion does not play a major role.
54.
Prosthetic treatment foredentulous patients, Zarb, Bolender, 12th edition , Syllabus of Complete denture, Charles M.
Heartwell, 4th edition
54
Adhesion and Xerostomia
Denture base seem to stick to the dry oral mucosa.
It is not very retentive and predisposes to mucosal abrasion and
ulcerations, due to lack of salivary lubrication.
It is annoying for the patients to have stick the denture base to the lips,
cheek and tongue.
55.
Prosthetic treatment foredentulous patients, Zarb, Bolender, 12th edition , Syllabus of Complete denture, Charles M.
Heartwell, 4th edition
55
Treatment for Xerostomia
An ethanol free rinse containing aloe or lanolin, a water soluble
lubricating jelly, or a salivary substitute containing
carboxymethylcellulose (CMC) or a mammalian mucin can be helpful.
In case or irradiation or autoimmune disorder; a prescription of 5 to 10 mg
of oral pilocarpine, 3 times a day can be beneficial if a patient can tolerate
the likely adverse effects like increased perspiration and occasionally
excess lacrimation.
56.
56
Cohesion
"the physicalattraction of like molecules for each other" - GPT
It acts within the thin film of saliva.
The effectiveness of these forces increases with increase in denture-
bearing area.
Prosthetic treatment for edentulous patients, Zarb, Bolender, 12th edition , Syllabus of Complete denture, Charles M.
Heartwell, 4th edition
57.
Prosthetic treatment foredentulous patients, Zarb, Bolender, 12th edition , Syllabus of Complete denture, Charles M.
Heartwell, 4th edition
57
Watery serous saliva can form a thinner film and is more cohesive than
thick mucous saliva.
Actually, normal saliva is not very cohesive.
58.
Prosthetic treatment foredentulous patients, Zarb, Bolender, 12th edition , Syllabus of Complete denture, Charles M.
Heartwell, 4th edition
58
Oral and Facial Musculature
It supply supplementary retentive forces, provided.
Teeth being positioned in the neutral zone.
Polished surface being properly shaped. This is not to say that patient
should hold their prosthetic teeth in place by conscious effort but the
shape of the buccal and lingual flanges must make it possible for the
musculature to fit automatically against the denture and thereby to
reinforce the border seal.
59.
Prosthetic treatment foredentulous patients, Zarb, Bolender, 12th edition , Syllabus of Complete denture, Charles M.
Heartwell, 4th edition
59
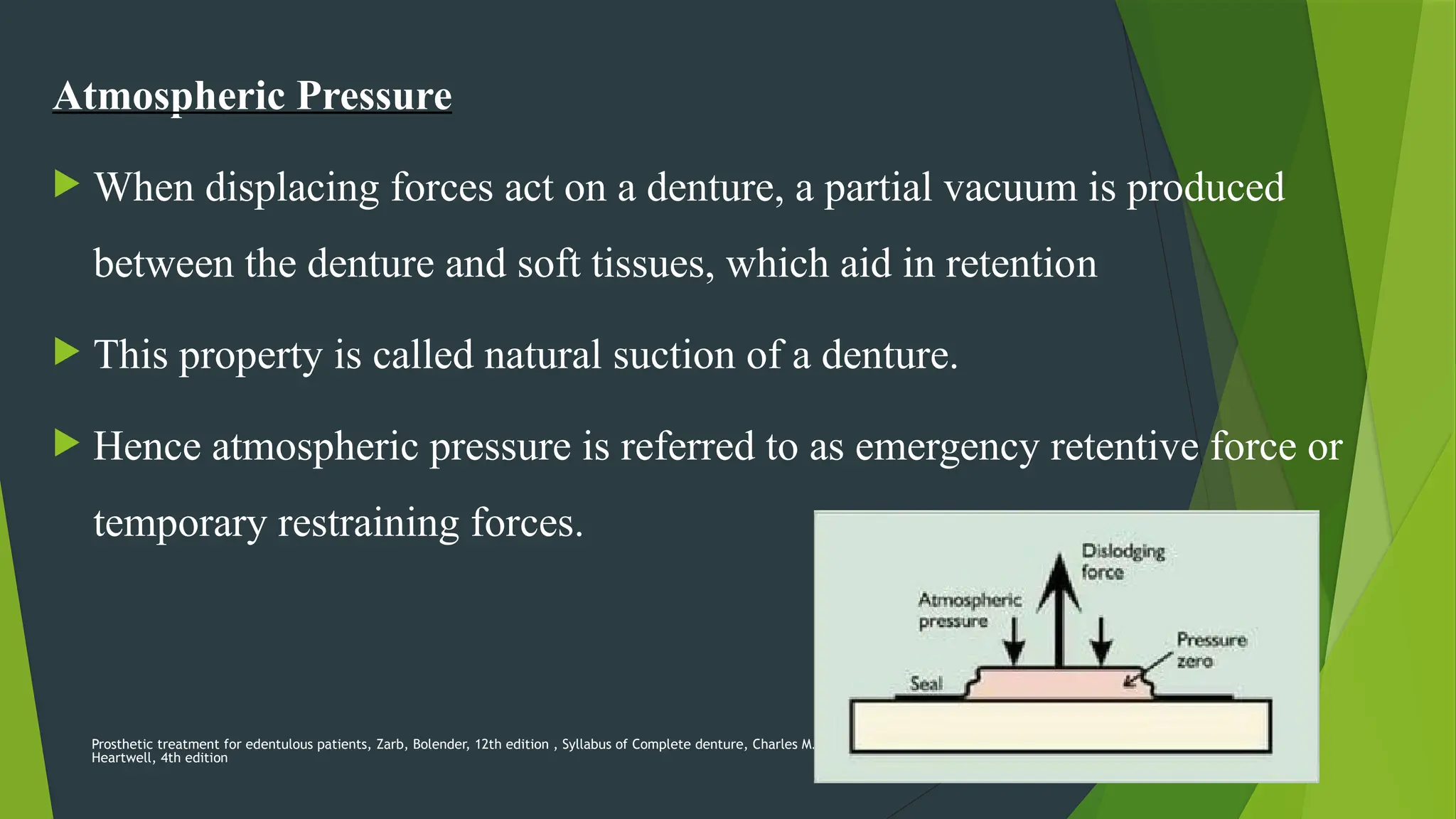
Atmospheric Pressure
When displacing forces act on a denture, a partial vacuum is produced
between the denture and soft tissues, which aid in retention
This property is called natural suction of a denture.
Hence atmospheric pressure is referred to as emergency retentive force or
temporary restraining forces.
60.
Prosthetic treatment foredentulous patients, Zarb, Bolender, 12th edition , Syllabus of Complete denture, Charles M.
Heartwell, 4th edition
60
Retention produced by an atmospheric pressure is directly proportional to
the denture base area.
61.
Prosthetic treatment foredentulous patients, Zarb, Bolender, 12th edition , Syllabus of Complete denture, Charles M.
Heartwell, 4th edition
61
Undercuts, Rotation insertion paths and Parallel walls.
The resiliency of the mucosa, submucosa overlying basal bone allows for
the existence of the modest undercut that can enhance retention.
Less severe undercuts of the lateral tuberosities, maxillary premolar areas,
distolingual areas and lingual mandibular midbody areas can be extremely
helpful to the retention of the prosthesis.
62.
Prosthetic treatment foredentulous patients, Zarb, Bolender, 12th edition , Syllabus of Complete denture, Charles M.
Heartwell, 4th edition
62
Some "undercuts" are only undercut in relationship to a linear path of
insertion or presumed vertical path of insertion.
However , if the undercut is seated first and the remainder of the denture
base can be brought into proximity with the basal seat on rotation of the
prosthesis around the undercut part that is already seated , this rotational
path will provide resistance against vertical displacement.
63.
Prosthetic treatment foredentulous patients, Zarb, Bolender, 12th edition , Syllabus of Complete denture, Charles M.
Heartwell, 4th edition
63
Prominent alveolar ridge with parallel and buccal walls may provide
significant retention by increasing the surface area between denture
and mucosa and thereby maximizing interfacial and atmospheric
forces.
64.
Prosthetic treatment foredentulous patients, Zarb, Bolender, 12th edition , Syllabus of Complete denture, Charles M.
Heartwell, 4th edition
64
Gravity
When a person is in upright posture, gravity acts as a retentive force for
the mandibular denture and a displacive force for the maxillary denture.
Weight of the denture acts as an important factor.
Curiously, another report focusing on maxillary denture base materials in
patients with xerostomia found strong patient preference for metal based
prothesis in the maxilla.
65.
Prosthetic treatment foredentulous patients, Zarb, Bolender, 12th edition , Syllabus of Complete denture, Charles M.
Heartwell, 4th edition
65
STABILITY
The stability of a denture is its ability to remain securely in place when
it is subjected to horizontal movements.
The latter occurs during the functional forces of chewing, talking,
singing, whistling, etc— all the orofacial activities needed for normal
everyday living.
66.
Prosthetic treatment foredentulous patients, Zarb, Bolender, 12th edition , Syllabus of Complete denture, Charles M.
Heartwell, 4th edition
66
To be stable, a denture requires:
• Good retention
• Noninterfering occlusion
• Proper tooth arrangement
• Proper form and contour of the polished surface
• Proper orientation of the occlusal plane
• Good control and coordination of the patient’s musculature.
67.
Prosthetic treatment foredentulous patients, Zarb, Bolender, 12th edition , Syllabus of Complete denture, Charles M.
Heartwell, 4th edition
67
Occlussion
No matter how skilfully the impressions were made, the dentures will
eventually loosen and cause irritation if there are interfering occlusal
contacts.
A common occurrence is an interfering contact in the second area that
may cause the mandibular denture to rotate upward and forward.
68.
68
Occlussal plane
• Ideallythe occlusal plane is parallel to and anatomically oriented to the
ridges.
• If the occlusal plane is tipped, there will be a shunting effect and a loss of
stability.
ESHETICS
The role of esthetics in impression making refers to the development of
the labial and buccal borders so that they are not only retentive but also
support the lips and cheeks properly.
Prosthetic treatment for edentulous patients, Zarb, Bolender, 12th edition , Syllabus of Complete denture, Charles M.
Heartwell, 4th edition
69.
Prosthetic treatment foredentulous patients, Zarb, Bolender, 12th edition , Syllabus of Complete denture, Charles M.
Heartwell, 4th edition
69
DISCUSSION
Pasad AK, Baviskar PS, Nadgere JB, Iyer JV. In 2021 Evaluated the
anxiety in patients undergoing complete denture treatment.
There is a greater need that the patient's expectations
be understood and their doubts, concerns and fears be lessened by proper
communication. Proper understanding of patient's mental attitude will help us
improve the approach of dentists towards complete denture treatment in a
more patient friendly way.
70.
Prosthetic treatment foredentulous patients, Zarb, Bolender, 12th edition , Syllabus of Complete denture, Charles M.
Heartwell, 4th edition
70
Shah U, Mahajan N, Bhatt N. in 2022 Evaluated Clinical evaluation of
complete denture fabricated using two different final impression
techniques on masticatory efficiency and oral health-related quality of
life.
Selective pressure and functional impression techniques
may be successfully used to fabricate complete dentures for patients with
resorbed ridges.
71.
Prosthetic treatment foredentulous patients, Zarb, Bolender, 12th edition , Syllabus of Complete denture, Charles M.
Heartwell, 4th edition
71
SH Cho, et al in 2015 evaluated the accuracy and reproducibility of a
digital impression and cast fabrication with a conventional impression
and cast fabrication.
They concluded that Compared with digital
impression and cast fabrication methods, conventional impression and cast
fabrication methods showed the statistically superior accuracy and
reproducibility.
72.
Prosthetic treatment foredentulous patients, Zarb, Bolender, 12th edition , Syllabus of Complete denture, Charles M.
Heartwell, 4th edition
72
CONCLUSION
Muller De Van stated that the perpetual
preservation of what remains is more important than the meticulous
replacement of what is lost.
73.
Prosthetic treatment foredentulous patients, Zarb, Bolender, 12th edition , Syllabus of Complete denture, Charles M.
Heartwell, 4th edition
73
REFERENCE
• Complete Denture Prosthodontics, John J. Sharry, 3rd edition
• Prosthetic treatment for edentulous patients, Zarb, Bolender, 12th edition.
• Syllabus of Complete denture, Charles M. Heartwell, 4th edition
• Glossary of Prosthodontic terms, 8th edition
• M. M, Devan, Basic principles in impression making, JPD 2005, 503-508
• Cho SH, Schaefer O, Thompson GA, Guentsch A. Comparison of accuracy and reproducibility of casts made
by digital and conventional methods. J Prosthet Dent. 2015
• Shah U, Mahajan N, Bhatt N. Clinical evaluation of complete denture fabricated using two different final
impression techniques on masticatory efficiency and oral health-related quality of life. J Indian Prosthodont
Soc. 2022 Oct-Dec;22
• Pasad AK, Baviskar PS, Nadgere JB, Iyer JV. Evaluation of anxiety in patients undergoing complete denture
treatment. J Indian Prosthodont Soc. 2021
74.
Prosthetic treatment foredentulous patients, Zarb, Bolender, 12th edition , Syllabus of Complete denture, Charles M.
Heartwell, 4th edition
74
THANK YOU