Downloaded 19 times

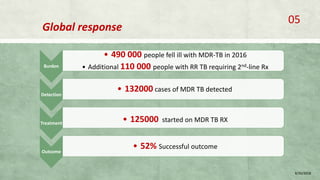
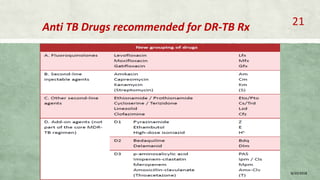
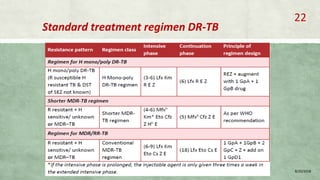
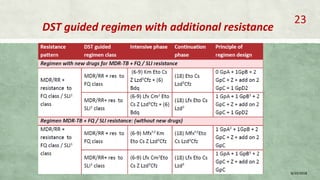
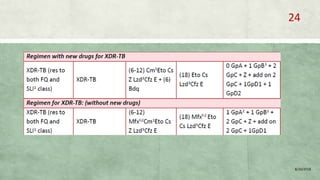
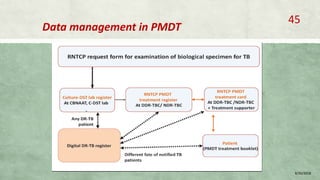
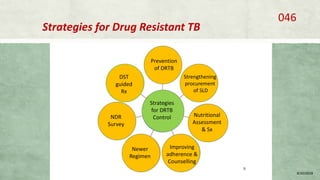


This document provides information on multi-drug resistant tuberculosis (MDR-TB), including its global and national burden, diagnosis, treatment, and management. Some key points include: - MDR-TB affects about 490,000 people globally each year and is a major public health issue, especially in countries like India, China, and Russia. - Diagnosis involves laboratory tests like phenotypic drug susceptibility testing (DST) or genotypic tests like line probe assays (LPA) and cartridge-based nucleic acid amplification tests (CBNAAT). DST guided treatment regimens are recommended. - Treatment of MDR-TB requires longer and more toxic drug regimens than drug-sensitive TB.



























































![ONFH[AVN HIP] -TRIPLE REGIME -A NOVAL SURGICAL CONCEPT .pptx](https://cdn.slidesharecdn.com/ss_thumbnails/onfhavnhip2026koaconcalicutdrgokuldevdrmashraf-260210064517-213ec005-thumbnail.jpg?width=640&height=640&fit=bounds)







![CTEV [ clubfoot] DR ARUN LAL ,DR MOHAMED ASHRAF travancore medical college k...](https://cdn.slidesharecdn.com/ss_thumbnails/ctevclubfootdrarunlaldrmohamedashraftravancoremedicalcollegekollamkeralaindia-260208063247-18fc466c-thumbnail.jpg?width=640&height=640&fit=bounds)



![PERI-PROSTHETIC FRACTURE NAIL-PLATE CONSTRUCT [NPC].pptx](https://cdn.slidesharecdn.com/ss_thumbnails/drarunkumardrmohamedashrafperiprostheticfrasturenail-plateconstructnpc-260209164459-7e9d15a1-thumbnail.jpg?width=640&height=640&fit=bounds)



