Childhood Maltreatment and PTSD Literature Review and Proposed StudyAlexandraPerkins5
This literature and proposed study explores several research articles relating to childhood maltreatment and PTSD. The second section proposes a hypothetical study to further explore a gap identified in the literature review.
Sample 3 bipolar on female adult populationNicole Valerio
Hello Sir
We are a premier academic writing agency with industry partners in UK, Australia and Middle East and over 15 years of experience. We are looking to establish long-term relationships with industry partners and would love to discuss this opportunity further with you.
Thanks & Regards
visit our website.
www.onlineassignmenthelp.com.au
www.freeassignmenthelp.com
www.btechndassignment.cheapassignmenthelp.co.uk
www.cheapassignmenthelp.com
www.cheapassignmenthelp.co.uk/
http://www.cheapassignmenthelp.net/
Childhood Maltreatment and PTSD Literature Review and Proposed StudyAlexandraPerkins5
This literature and proposed study explores several research articles relating to childhood maltreatment and PTSD. The second section proposes a hypothetical study to further explore a gap identified in the literature review.
Sample 3 bipolar on female adult populationNicole Valerio
Hello Sir
We are a premier academic writing agency with industry partners in UK, Australia and Middle East and over 15 years of experience. We are looking to establish long-term relationships with industry partners and would love to discuss this opportunity further with you.
Thanks & Regards
visit our website.
www.onlineassignmenthelp.com.au
www.freeassignmenthelp.com
www.btechndassignment.cheapassignmenthelp.co.uk
www.cheapassignmenthelp.com
www.cheapassignmenthelp.co.uk/
http://www.cheapassignmenthelp.net/
Religiosity and depression in college studentsDevon Berry
Presentation of study results examining relationship between depression and religiosity in college-age students. Background, methods, findings and discussion shared in brief format.
Children's longing for everydayness after tbiRichard Radecki
This is a interesting subject. Now, if sleep is disturbed after brain injury, which is not in my experienced addressed well in the acute phase of rehab, how about the "self". I've always stated that acute rehab is the simple time. Post-acute and community re-intergration has less resource dedication, knowledge, and research. Look at this article and try to grasp this struggle. With resource utilization focusing on movement there is still a paucity of effort on self and quality of life! Also note that this is reported as the first article looking at the individual for quality concepts.
A critical review of three articles reveals flawed empirical
evidence underpinning the case for integrating pharmacotherapy and
psychotherapy. Medical model dominance favors biology in a diathesis/
stress framework, creating myths of valid diagnosis, underlying biological
causes, and targeted pharmacological treatments. Meanwhile, a for-profit
pharmaceutical industry influences clinical trials, constructing an illusory
justification for medical intervention and bolstering the integration hypothesis.
The apparent logic of integration threatens to diminish the crucial,
empirically supported role of clients in psychotherapy outcome.
The authors call for the inclusion of client feedback in intervention
choices, based on accurate, unbiased information, and a continued critique
of pharmacotherapy
The art of being a failure as a therapist (haley, 1969)Scott Miller
A fantastic article written nearly 50 years ago that is as timely today as it was then. The author outlines several beliefs and practices sure to increase your chances of failing as a therapist.
Parent-infant interactions in families with women diagnosed with postnatal depression: a longitudinal study on the effects of a psychodynamic treatment
Religiosity and depression in college studentsDevon Berry
Presentation of study results examining relationship between depression and religiosity in college-age students. Background, methods, findings and discussion shared in brief format.
Children's longing for everydayness after tbiRichard Radecki
This is a interesting subject. Now, if sleep is disturbed after brain injury, which is not in my experienced addressed well in the acute phase of rehab, how about the "self". I've always stated that acute rehab is the simple time. Post-acute and community re-intergration has less resource dedication, knowledge, and research. Look at this article and try to grasp this struggle. With resource utilization focusing on movement there is still a paucity of effort on self and quality of life! Also note that this is reported as the first article looking at the individual for quality concepts.
A critical review of three articles reveals flawed empirical
evidence underpinning the case for integrating pharmacotherapy and
psychotherapy. Medical model dominance favors biology in a diathesis/
stress framework, creating myths of valid diagnosis, underlying biological
causes, and targeted pharmacological treatments. Meanwhile, a for-profit
pharmaceutical industry influences clinical trials, constructing an illusory
justification for medical intervention and bolstering the integration hypothesis.
The apparent logic of integration threatens to diminish the crucial,
empirically supported role of clients in psychotherapy outcome.
The authors call for the inclusion of client feedback in intervention
choices, based on accurate, unbiased information, and a continued critique
of pharmacotherapy
The art of being a failure as a therapist (haley, 1969)Scott Miller
A fantastic article written nearly 50 years ago that is as timely today as it was then. The author outlines several beliefs and practices sure to increase your chances of failing as a therapist.
Parent-infant interactions in families with women diagnosed with postnatal depression: a longitudinal study on the effects of a psychodynamic treatment
Cognitive Behavioral Treatments for Anxietyin Children With WilheminaRossi174
Cognitive Behavioral Treatments for Anxiety
in Children With Autism Spectrum Disorder
A Randomized Clinical Trial
Jeffrey J. Wood, PhD; Philip C. Kendall, PhD; Karen S. Wood, PhD; Connor M. Kerns, PhD;
Michael Seltzer, PhD; Brent J. Small, PhD; Adam B. Lewin, PhD; Eric A. Storch, PhD
IMPORTANCE Anxiety is common among youth with autism spectrum disorder (ASD), often
interfering with adaptive functioning. Psychological therapies are commonly used to treat
school-aged youth with ASD; their efficacy has not been established.
OBJECTIVE To compare the relative efficacy of 2 cognitive behavioral therapy (CBT) programs
and treatment as usual (TAU) to assess treatment outcomes on maladaptive and interfering
anxiety in children with ASD. The secondary objectives were to assess treatment outcomes
on positive response, ASD symptom severity, and anxiety-associated adaptive functioning.
DESIGN, SETTING, AND PARTICIPANTS This randomized clinical trial began recruitment in
April 2014 at 3 universities in US cities. A volunteer sample of children (7-13 years) with ASD
and maladaptive and interfering anxiety was randomized to standard-of-practice CBT,
CBT adapted for ASD, or TAU. Independent evaluators were blinded to groupings. Data
were collected through January 2017 and analyzed from December 2018 to February 2019.
INTERVENTIONS The main features of standard-of-practice CBT were affect recognition,
reappraisal, modeling/rehearsal, in vivo exposure tasks, and reinforcement. The CBT
intervention adapted for ASD was similar but also addressed social communication and
self-regulation challenges with perspective-taking training and behavior-analytic techniques.
MAIN OUTCOMES AND MEASURES The primary outcome measure per a priori hypotheses was
the Pediatric Anxiety Rating Scale. Secondary outcomes included treatment response on the
Clinical Global Impressions–Improvement scale and checklist measures.
RESULTS Of 214 children initially enrolled, 167 were randomized, 145 completed treatment,
and 22 discontinued participation. Those who were not randomized failed to meet eligibility
criteria (eg, confirmed ASD). There was no significant difference in discontinuation rates
across conditions. Randomized children had a mean (SD) age of 9.9 (1.8) years; 34 were
female (20.5%). The CBT program adapted for ASD outperformed standard-of-practice CBT
(mean [SD] Pediatric Anxiety Rating Scale score, 2.13 [0.91] [95% CI, 1.91-2.36] vs 2.43 [0.70]
[95% CI, 2.25-2.62]; P = .04) and TAU (2.93 [0.59] [95% CI, 2.63-3.22]; P < .001). The CBT
adapted for ASD also outperformed standard-of-practice CBT and TAU on parent-reported
scales of internalizing symptoms (estimated group mean differences: adapted vs
standard-of-practice CBT, −0.097 [95% CI, −0.172 to −0.023], P = .01; adapted CBT vs TAU,
−0.126 [95% CI, −0.243 to −0.010]; P = .04), ASD-associated social-communication
symptoms (estimated group mean difference: adapted vs standard-of-practice CBT, −0.115
[95% CI, −0223 to −0 ...
· Journal List
· HHS Author Manuscripts
· PMC5626643
J Affect Disord. Author manuscript; available in PMC 2019 Jan 1.
Published in final edited form as:
J Affect Disord. 2018 Jan 1; 225: 395–398.
Published online 2017 Aug 15. doi: 10.1016/j.jad.2017.08.023
PMCID: PMC5626643
NIHMSID: NIHMS902372
PMID: 28850853
Quantitative genetic analysis of anxiety trait in bipolar disorder
J Contreras,1 E Hare,3 G Chavarría,2 and H Raventós1,2
Author informationCopyright and License informationDisclaimer
The publisher's final edited version of this article is available at J Affect Disord
See other articles in PMC that cite the published article.
Go to:
Abstract
Background
Bipolar disorder type I (BPI) affects approximately 1% of the world population. Although genetic influences on bipolar disorder are well established, identification of genes that predispose to the illness has been difficult. Most genetic studies are based on categorical diagnosis. One strategy to overcome this obstacle is the use of quantitative endophenotypes, as has been done for other medical disorders.
Methods
We studied 619 individuals, 568 participants from 61 extended families and 51 unrelated healthy controls. The sample was 55% female and had a mean age of 43.25 (SD 13.90; range 18–78).
Heritability and genetic correlation of the trait scale from the Anxiety State and Trait Inventory (STAI) was computed by using the general linear model (SOLAR package software).
Results
we observed that anxiety trait meets the following criteria for an endophenotype of bipolar disorder type I (BPI): 1) association with BPI (individuals with BPI showed the highest trait score (F=15.20 [5,24], p=0.009), 2) state-independence confirmed after conducting a test-retest in 321 subjects, 3) co-segregation within families 4) heritability of 0.70 (SE: 0.060), p=2.33×10−14 and 5) genetic correlation with BPI was 0.20, (SE=0.17, p=3.12×10−5).
Limitations
Confounding factors such as comorbid disorders and pharmacological treatment could affect the clinical relationship between BPI and anxiety trait. Further research is needed to evaluate if anxiety traits are specially related to BPI in comparison with other traits such as anger, attention or response inhibition deficit, pathological impulsivity or low self-directedness.
Conclusions
Anxiety trait is a heritable phenotype that follows a normal distribution when measured not only in subjects with BPI but also in unrelated healthy controls. It could be used as an endophenotype in BPI for the identification of genomic regions with susceptibility genes for this disorder.
Keywords: Bipolar disorder, Endophenotype, Genetics, Heritability, Anxiety, Central Valley of Costa Rica
Go to:
Introduction
Estimates of the prevalence of bipolar I disorder have ranged from 0.8% to 1.6% of the general population (Berns and Nemeroff, 2003). Although the genetic participation is well established, the identification of genes has remained elusive. Imprecision of the phenotype might ...
· Journal List
· HHS Author Manuscripts
· PMC5626643
J Affect Disord. Author manuscript; available in PMC 2019 Jan 1.
Published in final edited form as:
J Affect Disord. 2018 Jan 1; 225: 395–398.
Published online 2017 Aug 15. doi: 10.1016/j.jad.2017.08.023
PMCID: PMC5626643
NIHMSID: NIHMS902372
PMID: 28850853
Quantitative genetic analysis of anxiety trait in bipolar disorder
J Contreras,1 E Hare,3 G Chavarría,2 and H Raventós1,2
Author informationCopyright and License informationDisclaimer
The publisher's final edited version of this article is available at J Affect Disord
See other articles in PMC that cite the published article.
Go to:
Abstract
Background
Bipolar disorder type I (BPI) affects approximately 1% of the world population. Although genetic influences on bipolar disorder are well established, identification of genes that predispose to the illness has been difficult. Most genetic studies are based on categorical diagnosis. One strategy to overcome this obstacle is the use of quantitative endophenotypes, as has been done for other medical disorders.
Methods
We studied 619 individuals, 568 participants from 61 extended families and 51 unrelated healthy controls. The sample was 55% female and had a mean age of 43.25 (SD 13.90; range 18–78).
Heritability and genetic correlation of the trait scale from the Anxiety State and Trait Inventory (STAI) was computed by using the general linear model (SOLAR package software).
Results
we observed that anxiety trait meets the following criteria for an endophenotype of bipolar disorder type I (BPI): 1) association with BPI (individuals with BPI showed the highest trait score (F=15.20 [5,24], p=0.009), 2) state-independence confirmed after conducting a test-retest in 321 subjects, 3) co-segregation within families 4) heritability of 0.70 (SE: 0.060), p=2.33×10−14 and 5) genetic correlation with BPI was 0.20, (SE=0.17, p=3.12×10−5).
Limitations
Confounding factors such as comorbid disorders and pharmacological treatment could affect the clinical relationship between BPI and anxiety trait. Further research is needed to evaluate if anxiety traits are specially related to BPI in comparison with other traits such as anger, attention or response inhibition deficit, pathological impulsivity or low self-directedness.
Conclusions
Anxiety trait is a heritable phenotype that follows a normal distribution when measured not only in subjects with BPI but also in unrelated healthy controls. It could be used as an endophenotype in BPI for the identification of genomic regions with susceptibility genes for this disorder.
Keywords: Bipolar disorder, Endophenotype, Genetics, Heritability, Anxiety, Central Valley of Costa Rica
Go to:
Introduction
Estimates of the prevalence of bipolar I disorder have ranged from 0.8% to 1.6% of the general population (Berns and Nemeroff, 2003). Although the genetic participation is well established, the identification of genes has remained elusive. Imprecision of the phenotype might ...
O R I G I N A L P A P E RSelf-Reported Depressive Symptoms.docxhopeaustin33688
O R I G I N A L P A P E R
Self-Reported Depressive Symptoms Have Minimal Effect
on Executive Functioning Performance in Children
and Adolescents
Benjamin D. Hill • Danielle M. Ploetz •
Judith R. O’Jile • Mary Bodzy • Karen A. Holler •
Martin L. Rohling
Published online: 9 May 2012
� Springer Science+Business Media, LLC 2012
Abstract The relation between mood and executive
functioning in children and adolescents has not been previ-
ously reported. This study examined the association between
self-reported depressive symptoms in both clinical outpa-
tient and psychiatric inpatient samples to the following
measures of executive functioning: the Controlled Oral
Word Association Test, Animal Naming, Trail Making Test,
and Wisconsin Card Sorting Test. Records from children and
adolescents aged 7–17 years old with an IQ [ 70 were
examined. Data were gathered at either an outpatient neu-
ropsychology clinic (n = 89) or an inpatient psychiatric
hospital setting (n = 81). Mood was measured with the
Children’s Depression Inventory. Generally, statistical
associations between self-reported depressive symptoms and
executive functioning were small and non-significant. The
variance predicted by mood on measures of executive
functioning was minimal (generally less than 2 %) for the
total sample, the outpatient group, inpatient group, and a
subgroup who endorsed elevated mood symptoms. These
results suggest that impaired performance on measures of
executive functioning in children and adolescents is mini-
mally related to self-reported depressive symptoms.
Keywords Executive functioning � Mood � Depression �
Cognitive ability � Neuropsychological assessment
Introduction
There is a long standing debate that has generated a con-
siderable amount of research in adults concerning the
relationship between levels of emotional disturbance and
their effects on performance on standard neuropsycholog-
ical tests. It appears that when the literature is taken as a
whole, adults diagnosed with psychiatric disorders tend to
perform worse than individuals without diagnoses (Basso
and Bornstein 1999; Cassens et al. 1990; Kindermann and
Brown 1997; Sackeim et al. 1992; Sherman et al. 2000;
Sweet et al. 1992; Tancer et al. 1990; Veiel 1997).
Depression, the most common mood disorder, is generally
associated with dysfunctional memory performance in the
adult literature (Burt et al. 1995; Christensen et al. 1997).
However, adult studies have shown conflicting patterns of
results across other neuropsychological domains. Some
researchers have reported depression to also be associated
with executive dysfunction (McDermott and Ebmeier
2009; Reppermund et al. 2007; Merriam et al. 1999; Martin
et al. 1991). However, others studies have reported no
effect of depression on executive functioning (Castaneda
et al. 2008; Miller et al. 1991; Rohling et al. 2002, Markela-
Lerenc et al. 2006).
While many different adult populations have been
.
11. Identifying the Elements of the Limitations & ImplicationsGo tBenitoSumpter862
11. Identifying the Elements of the Limitations & Implications
Go to the Limitations/Implications section(s) and identify the limitations of the study and how those limitations impacted the whole study.
12. Identifying the Elements of the Conclusion Section
Go to the Conclusion section and identify the conclusive statements of the study and the recommendations made for future research.
POST # 1 EDITHA
When assessing an adolescent with bipolar disorder, what are some of the diagnostic and treatment challenges the clinician might face?
Bipolar disorder is a serious mental health disorder that is often first diagnosed during young adulthood or adolescence. Symptoms of the illness, however, also can appear in early childhood. Although once thought rare in children, diagnosis of bipolar disorder in children has significantly increased over the last decade (Papolos & Bronsteen, 2018). Despite the increased diagnosis of bipolar disorder in children, assessment and diagnosis remain challenging and controversial. This is, in part, because of the lack of research on this disorder in children and adolescents and the growing recognition that the disease can present differently in children from how it presents in adults (AACAP, 2019). Over the years, more attention has focused on the unique presentation of bipolar disorder in the young that has introduced new ways of looking at this disease and assessing it in children.
The importance of identifying the presence of bipolar disease at an early age is highlighted by data showing that adults in whom bipolar disease started at an early age have a more severe course of the illness compared with adult-onset disease. Early-onset disease is associated with a higher risk of suicide; severe mood lability and polarity; lower quality of life and greater functional impairment; higher rates of comorbidity; and a higher risk of substance use disorders compared with adult-onset disease (Papolos & Bronsteen, 2018). Although some children meet the criteria established for adults categorized in the DSM-5, many children fall outside these classical categories, and diagnosis in these children is particularly challenging and difficult (APA, 2013). For these children, additional information beyond what is provided in the DSM may help make an accurate diagnosis which causes increased challenges in assessment and diagnosis.
References
Papolos, D, & Bronsteen A. (2018) bipolar disorder in children: assessment in general pediatric practice. Curr Opin Pediatr, 25(3):419-426.
American Academy of Child and Adolescent Psychiatry (AACAP). (2019) bipolar disorder: Parents’ Medication Guide for Bipolar Disorder in Children & Adolescents.
American Psychiatric Association (APA) (2013). Diagnostic and Statistical Manual of Mental Disorders, Fifth Edition (DSM-5). Washington, DC: American Psychiatric Association.
RESEARCH ARTICLE
Association of suicidal behavior with exposure
to suicide and suicide attempt: A systematic
...
11. Identifying the Elements of the Limitations & ImplicationsGo tSantosConleyha
11. Identifying the Elements of the Limitations & Implications
Go to the Limitations/Implications section(s) and identify the limitations of the study and how those limitations impacted the whole study.
12. Identifying the Elements of the Conclusion Section
Go to the Conclusion section and identify the conclusive statements of the study and the recommendations made for future research.
POST # 1 EDITHA
When assessing an adolescent with bipolar disorder, what are some of the diagnostic and treatment challenges the clinician might face?
Bipolar disorder is a serious mental health disorder that is often first diagnosed during young adulthood or adolescence. Symptoms of the illness, however, also can appear in early childhood. Although once thought rare in children, diagnosis of bipolar disorder in children has significantly increased over the last decade (Papolos & Bronsteen, 2018). Despite the increased diagnosis of bipolar disorder in children, assessment and diagnosis remain challenging and controversial. This is, in part, because of the lack of research on this disorder in children and adolescents and the growing recognition that the disease can present differently in children from how it presents in adults (AACAP, 2019). Over the years, more attention has focused on the unique presentation of bipolar disorder in the young that has introduced new ways of looking at this disease and assessing it in children.
The importance of identifying the presence of bipolar disease at an early age is highlighted by data showing that adults in whom bipolar disease started at an early age have a more severe course of the illness compared with adult-onset disease. Early-onset disease is associated with a higher risk of suicide; severe mood lability and polarity; lower quality of life and greater functional impairment; higher rates of comorbidity; and a higher risk of substance use disorders compared with adult-onset disease (Papolos & Bronsteen, 2018). Although some children meet the criteria established for adults categorized in the DSM-5, many children fall outside these classical categories, and diagnosis in these children is particularly challenging and difficult (APA, 2013). For these children, additional information beyond what is provided in the DSM may help make an accurate diagnosis which causes increased challenges in assessment and diagnosis.
References
Papolos, D, & Bronsteen A. (2018) bipolar disorder in children: assessment in general pediatric practice. Curr Opin Pediatr, 25(3):419-426.
American Academy of Child and Adolescent Psychiatry (AACAP). (2019) bipolar disorder: Parents’ Medication Guide for Bipolar Disorder in Children & Adolescents.
American Psychiatric Association (APA) (2013). Diagnostic and Statistical Manual of Mental Disorders, Fifth Edition (DSM-5). Washington, DC: American Psychiatric Association.
RESEARCH ARTICLE
Association of suicidal behavior with exposure
to suicide and suicide attempt: A systematic
...
1Running Head FINAL PROPOSAL CHILD ABUSE AND ADULT MENTAL HEAL.docxdrennanmicah
1
Running Head: FINAL PROPOSAL: CHILD ABUSE AND ADULT MENTAL HEALTH
2
FINAL PROPOSAL: CHILD ABUSE AND ADULT MENTAL HEALTH
Diamond Newton
Southern New Hampshire University
March 3, 2019
Problem Statement
Several adults struggle from a variety of mental health issues (suicidal thoughts and tendencies, alcoholism, depression, and drug abusers.) A lot of those issues may stem from what took place during an adult’s childhood that stem from a variety of reasons. Some adults seek help and some refuse to seek help. The adults who do seek help come to realize that their current issues stem from when they were a child and still developing as a human. Child abuse can come in many forms, physical, mental, and sexual. Adults who have been exposed or experienced this are likely to suffer from some form of mental health issue. It is important to figure out the root of mental health issues in adults so the root can be addressed. Children need to be in a healthy environment with nothing short of love and care. Exposing children to a harsh reality is only breeding them into an adult who suffers from mental health issues.
Literature Review
The study of psychology helps researchers to understand better what is going on with a person. Researchers studied what happened in a person's life that causes them to make the decisions they do and behave in a certain way. Adults have this stigmatism that they can do whatever they want because they are "grown." Many adults suffer from something that can cause to lead towards suicidal thoughts and tendencies, alcoholism, depression, and drug abusers. A lot of those issues may stem from what took place during an adult’s childhood. There could be some reasons adults tend to display certain mental health traits that have been studied in many different forms by researchers. What we will be reviewed is the abuse, physical or mental, that an adult endured as a child and how it affects them in their adulthood.
Blanco, C., Grant, B. F., Hasin, D. S., Lin, K. H., Olfson, M. Sugaya, L. (2012) recognized that child physical abuse had been associated with an increased risk of suicide attempts. The study conducted included Blacks, Hispanics and young adults between the ages of 18-24 in 2001-2002 and 2004-2005. In person, interviews were conducted in Wave 1. In Wave 2 used similar methods as Wave 1 but it excluded the individuals who were not eligible. Wave 2 also interviews went into depth about the questions asked for the participants first 17 years of life. There are many other variables that have been added to the data that relate to childhood physical abuse and mental health distress in adult years. Those other adversatives included the history of child sexual abuse and neglect, parental psychopathology, and perceived parental support, described as emotional neglect.
The advantages to this design would be the inclusion of other childhood adversities that could contribute to adult psychiatri.
Unit III PowerPoint Presentation Develop a PowerPoint Presentat.docxmarilucorr
Unit III PowerPoint Presentation
Develop a PowerPoint Presentation about standards/code sets, and include a slide for each topic outlined below:
· Slide 1: Introduction
· Slide 2: ICD 9 Overview
· Slide 3: ICD 10 Overview
· Slide 4: ICD 9 and ICD 10 Compare and Contrast
· Slide 5: Describe a SNOMED-CT Code
· Slide 6: Describe a NDC
· Slide 7: Describe a CDT
· Slide 8: Discuss why code sets are used
· Slide 9: Summary slide
· Slide 10: Reference slide with at least one outside source, not counting the textbook
MUST BE IN APA FORMAT
If you need additional space for a slide, please use the notes section under the slide.
Running head: CHILD SURVIVORS OF TRAUMATIC STRESS 1
CHILD SURVIVORS OF TRAUMATIC STRESS 2
Annotated Bibliography: Child who are Survivors of Traumatic Stress
name
school
2 July 2016
Annotated Bibliography: Child who are Survivors of Traumatic Stress
Neugebauer, R., Fisher, P. W., Turner, J. B., Yamabe, S., Sarsfield, J. A., & Stehling-Ariza, T. (2009). Post-traumatic stress reactions among Rwandan children and adolescents in the early aftermath of genocide. International journal of epidemiology, 38(4), 1033-1045.
The study surveyed Rwandese children aged between 8 and 19 to measure traumatic exposures using an inventory of possible war time encounters and post-traumatic stress reactions against a checklist of symptoms of PTSD. Those who meet the assessed PTSD diagnosis model are categorized as the cases of probable PTSD. In a sample of 1547, the participants were divided into two. The respondents were exposed to horrific experiences during the war including witnessing killings, rape, sexual mutilation, and in some cases hiding under the corpse. In the two groups of respondents, the study has determined that the rate of probable PTSD was 62% and 54% in the first and second samples respectively. Some of the individuals had the rate that is as high as 100%. Besides, the study found out that the rate of probable PTSD was higher in women than in men. Still, the result indicates that the test on age gave inconsistent.
Wasserman, G. A., McReynolds, L. S., Lucas, C. P., Fisher, P., & Santos, L. (2002). The voice DISC-IV with incarcerated male youths: prevalence of disorder. Journal of the American Academy of Child & Adolescent Psychiatry, 41(3), 314-321.
The scholars intended to assess the rate of psychiatric disorder amongst the incarcerated youths. Also, they had the objective of examining the feasibility of applying a self administered and comprehensive structured psychiatric evaluation of the incarcerated juveniles. The youths, parents, and staff tolerated well the assessments with 92% of the approached juveniles agreeing. Above the expectable higher levels of substance use and disruptive disorders, the juveniles indicated high levels of mood and anxiety disorders, with above 3% of th ...
1PAGE 21. What is the question the authors are asking .docxfelicidaddinwoodie
1
PAGE
2
1. What is the question the authors are asking?
They asked about a reduction in judgmental biases regarding the cost and probability associated with adverse social events as they are presumed as being mechanisms for the treatment of Social Anxiety Disorder (SAD). Also, the authors poised on the changes in judgmental biases as mechanisms to explain cognitive-behavioral therapy for social anxiety disorder. On top of that, they stated that methodological limitations extant studies highlight the possibility that rather than causing symptom relief, a significant reduction in judgmental biases tends to be consequences of it or correlate. Considerably, they expected cost bias at mid-treatment to be a predictor of the treatment outcome.
2. Why do the authors believe this question is important?
According to the authors, this question was relevant as methodological limitations of present studies reflect on the possibility that instead of causing symptom belief, a significant reduction in judgmental biases can be consequences or correlated to it. Additionally, they ought to ascertain the judgment bias between treated and non-treated participants. Significantly, this was important as they had to determine the impact of pre and post changes in cost and probability of the treatment outcomes. But, probability bias at mid-treatment was a predictor of the treatment outcome contrary to the cost bias at mid-treatment that could not be identified as a significant predictor of the treatment outcome.
3. How do they try to answer this question?
They conducted a study to evaluate the significant changes in judgmental bias as aspects of cognitive-behavioral therapy for social anxiety disorders. To do this, they conducted a study using information from two treatment studies; an uncontrolled trial observing amygdala activity as a response to VRE (Virtual Reality Exposure Therapy) with the use of functional magnetic resonance imaging and a randomized control trial that compared Virtual Reality Exposure Therapy with Exposure Group Therapy for SAD. A total of 86 individuals who met the DSM-IV-TR criteria for the diagnosis of non-generalized (n=46) and generalized (n=40) SAD participated. After completing eight weeks of the treatment protocol, the participants who identified public speaking as their most fearsome social situation were included. The SCID (Structured clinical interview for the DSM-IV) was used to ascertain diagnostic and eligibility status on Axis 1 conditions within substance abuse, mood and anxiety disorder modules. The social anxiety measures were measured with the use of BFNE (Brief Fear of Negative Evaluation), a self-reporting questioner that examined the degree to which persons fear to be assessed by other across different social settings. Additionally, the OPQ (Outcome Probability Questionnaire) self-reporting questionnaire was used to evaluate individual’s estimate on the probability that adverse, threatening events will occur at t ...
Research-Based Interventions: Dissociative Identity Disorder 1
THIS IS AN EXAMPLE PLEASE DO NO COPY DO NOT PLAGiarism
Research-Based Interventions: Dissociative Identity Disorder
“Dissociative identity disorder is characterized by the presence of two or more identities or personality states, each with its relatively enduring pattern of perceiving, relating to, and thinking about the environment and the self” (Vermetten, Schmahl, Lindner, Loewenstein, & Bremner, 2006). There are many characteristics used that accompany Dissociative Disorder (DID). One method to understanding would be to know how the disorders are classified and defined. DID may be conceptualized effectively using the diathesis-stress model. There are many different intervention strategies for this disorder as well. Over time researchers have discovered the most effective treatments and interventions that can be used regarding DID. When one dissociates, the person may not have conscious awareness of what is happening (Vermetten, Schmahl, Lindner, Loewenstein, & Bremner, 2006).
Peer-reviewed Articles
One limitless, longitudinal, naturalistic, and prospective study investigated childhood maltreatment (CM) in adult intimate partner violence (IPV) victims among Dissociative Disorder (DD) patients with Dissociative Identity Disorder with CM rates of 80-95% and severe dissociative symptoms (Webermann, Brand, & Chasson, 2014). The methods of this study include 275 DD outpatient therapy patients who completed a self-reported measure of dissociation (Webermann, Brand, & Chasson, 2014). Analyses assessed associations between CM typologies, trait dissociation, and IPV (Webermann, Brand, & Chasson, 2014). The results of this study include emotional and physical child abuse associated with childhood witnessing of domestic violence, physical, and emotional IPV (Webermann, Brand, & Chasson, 2014) Two-tailed independent samples t -tests and z-tests were used in this study to represent data as well. “As an effect size, odds ratios (ORs) were calculated to predict the likelihood of a participant being in an abusive adult relationship if they experienced a particular type of CM” (Webermann, Brand, & Chasson, 2014, p. 5).
A double-blind study was conducted including 15 females with DID compared to 23 without psychopathology., chosen by self-disclosure results of a questionnaire along with a structured clinical interview by psychiatrists The objective was to examine the volumetric differences between amygdala and hippocampal volumes in patients with dissociative identity disorder, a disorder that has been associated with a history of severe childhood trauma (Vermetten, Schmahl, Lindner, Loewenstein, & Bremner, 2006). These researchers used MRI to measure volumes of the amygdala and hippocampus. The results included the volume of the hippocampus being 19.2 % smaller and the amygdala being 31.6% smaller in patients with DID when compared to the other subjects without psychopath ...
Association Between Participant-Identified Problems And Depression Severity I...
MPA Poster_Rapoport
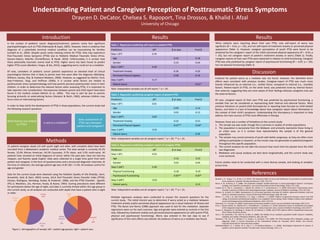
1. Understanding Patient and Caregiver Perception of Posttraumatic Stress Symptoms
Draycen D. DeCator, Chelsea S. Rapoport, Tina Drossos, & Khalid I. Afzal
University of Chicago
Introduction
Methods
Table 1. Regression predicting self-report or patient PTSS
Predictors ΔR2 β at step Final β
Step 1 (R2) 0.34
Age -0.10 -0.18
Gender 0.33 -0.04
Step 2 (ΔR2) 0.30
Treatment Anxiety -0.36 -0.20
Perceived Physical Appear. -0.38 -0.16
Step 3 (ΔR2) 0.17
Patient worry -0.61*
Results
Discussion
References
Caucasia
n
63%
African
America
n
23%
Asian
14%
8-12yo
25%
13-17yo
29%
18-25yo
46%
Figure 1. Demographics of sample; left = patient age groups; right = patient race.
Note. Independent variables are all self-report; * p < .05.
Table 2. Regression predicting caregiver-report of patient PTSS
Predictors ΔR2 β at step Final β
Step 1 (R2) 0.01
Age -0.09 0.14
Gender 0.03 -0.12
Step 2 (ΔR2) 0.83
Treatment Anxiety -0.32 -0.31
Perceived Physical Appear. -0.67** -0.64*
Step 3 (ΔR2) 0.01
Patient worry -0.05
Note. Independent variables are all caregiver-report; * p < .05; ** p < .01.
Table 3. Regression predicting caregiver-report of caregiver PTSS
Predictors ΔR2 β at step Final β
Step 1 (R2) 0.03
Age 0.16 0.23
Gender 0.03 -0.05
Step 2 (ΔR2) 0.49
Physical Functioning 0.18 0.19
Psychosocial Functioning -0.83** -0.87*
Step 3 (ΔR2) 0.01
Patient worry 0.12
Note. Independent variables are all caregiver-report; * p < .05; ** p < .01.
31 patient–caregiver dyads (19 with youth eight and older, with complete data) have been
recruited from a Midwestern academic medical center. The total sample is currently 45.2%
female, 22.6% African American, 64.5% Caucasian, 9.7% Asian, and 3.2% multi-racial. All
patients have received an initial diagnosis of cancer within the past year, have not had any
relapses, and fluently speak English. Data were collected at a single time point from both
patient and caregiver, in the form of questionnaires and a structured diagnostic interview. At
the time of collection, the average patient age was 14.81 (SD = 5.19). All analyses control for
age and gender.
Data for the current study were obtained using the Pediatric Quality of Life (PedsQL; Varni,
Burwinkle, Seid, & Skarr, 2003) survey, UCLA Post-Traumatic Stress Disorder Index (PTSDI;
Pynoos, Rodriguez, Steinberg, Stuber, & Frederick, 1998), and the PTSD Checklist - Specific
(PCL-S; Weathers, Litz, Herman, Huska, & Keane, 1993). Scoring procedures were different
for participants below the age of eight, and data is currently limited within this age group in
the current study, so all analyses are conducted with dyads that have a patient who is eight
or older.
In the context of pediatric cancer diagnosis/treatment, patients rarely face significant
psychopathologies such as PTSD (Patenaude & Kupst, 2005). However, there is evidence that
diagnosis of a potentially terminal medical condition can be traumatizing for families
(Landolt et al., 2002). Despite youth rarely meeting criteria for PTSD, they may experience
Post-Traumatic Stress Sympoms (PTSS) due to Pediatric Medical Traumatic Stress (Price,
Kassam-Adams, Alderfer, Christofferson, & Kazak, 2016). Unfortunately, it is unclear how
these potentially traumatic events lead to PTSS. Higher worry has been found to predict
higher PTSS scores (Bardeen, Fergus, & Wu, 2012), suggesting worry could act as a mediator.
Of note, caretakers of pediatric cancer patients experience an elevated level of clinical
psychological distress that is likely to persist even five years after the diagnosis (Wijnberg-
Williams, Kamps, Klip, & Hoekstra-Weebers, 2006). However, as suggested by Martin, Ford,
Dyer-Friedman, Tang, and Huffman (2004), it is unclear what factors are related to
posttraumatic stress symptomatology and how parents perceive posttraumatic stress in their
children. In order to determine the relevant factors when assessing PTSS, it is important to
take reporters into consideration. Discrepancies between parent and child report have been
found in the medical context (Martin et al., 2004). This may in part be due to parents
focusing primarily on externalizing factors (Herjanic & Reich, 1982), whereas children may
focus more on internalizing factors.
In order to help clarify the development of PTSS in these populations, the current study had
the following research questions:
Results
When patients were reporting about their own PTSS, only self-report of worry was
significant (β = -0.61, p < .05), and not self-report of treatment anxiety or perceived physical
appearance (Table 1). However, caregiver perceptions of youth PTSS were found to be
predicted by the caregiver’s report of the child’s perceived physical appearance (β = -0.63, p
< .05), but not caregiver report of patient’s treatment anxiety or worry (Table 2). Finally,
caregiver reports of their own PTSS were examined in relation to child functioning. Caregiver
PTSS was only predicted by caregiver report of psychosocial functioning (β = -0.87, p < .05),
but not physical functioning (Table 3).
Evidence for patient worry as a mediator was not found. However, the identified direct
effects were consistent with previous studies. Caregiver-report of PTSS was much more
heavily influenced by an external (i.e., visible) factor, compared to internal (i.e., invisible)
factors. Patient-report of PTSS, on the other hand, was predicted more by internal factors
than external, suggesting they are more aware of their feelings whereas caregivers only see
the external factors.
Of note, caregiver-report of their own PTSS was predicted by psychosocial functioning, a
variable that can be considered as representing both internal and external factors. Most
previous literature on parent-child discrepancies in reporting have focused on child-related
factors, and there is a lack of knowledge about how caregivers report about themselves in
the context of their child’s symptoms. Understanding this discrepancy is important to help
address the main sources of PTSS most effectively in therapy.
However, there are a number of limitations to the current study:
1. The sample size was small, though this is common in studies of similar populations.
2. The population is exclusively from the Midwest, and primarily represents those living in
an urban area, so it is unclear how representative the sample is of the general
population.
3. The sample may consist primarily of youth with better prognoses, as they are often more
willing to participate in research, so the results may not generalize to patients/caregivers
throughout this specific population.
4. The current analyses do not take into account how much time has passed since the child
was diagnosed.
5. Mediation and causal analyses are best done longitudinally, and the current study was
cross-sectional.
Future studies need to be conducted with a more diverse sample, and looking at variables
across time.
What factors are related
to PTSS?
Is worry a mediator?
Does assessment of
PTSS vary between
patient and caregiver?
Multiple regression analyses were conducted to answer the research questions for the
current study. The initial interest was to determine if worry acted as a mediator between
treatment anxiety and/or perceived physical appearance (as a visual indicator of illness) and
PTSS. The Baron and Kenny (1986) approach was used to test for this mediation. Separate
regressions were run for each outcome. Age and gender were entered as controls in the first
step, followed by treatment anxiety and perceived physical appearance (or with parent PTSS,
physical and psychosocial functioning). Worry was entered in the last step to see if
significance of the main effects was altered. No evidence of worry as a mediator was found.
Bardeen, J. R., Fergus, T. A., & Wu, K. D. (2012). The interactive effect of worry and intolerance of uncertainty on posttraumatic
stress symptoms. Cognitive Therapy and Research, 37(4), 742–751.
Baron, R. M., & Kenny, D. A. (1986). The moderator-mediator variable distinction in social psychological research: Conceptual,
strategic, and statistical considerations. Journal of Personality and Social Psychology, 51(6), 1173–1182.
Landolt, M. A., Ribi, K., Laimbacher, J., Vollrath, M., Gnehm, H. E., & Sennhauser, F. H. (2002). Brief report: Posttraumatic Stress
Disorder in parents of children with newly diagnosed type 1 diabetes. Journal of Pediatric Psychology, 27(7), 647–652.
Herjanic, B., & Reich, W. (1982). Development of a structured psychiatric interview for children: Agreement between child and
parent on individual symptoms. Journal of Abnormal Child Psychology, 10(3), 307–324.
Martin, J. L., Ford, C. B., Dyer-Friedman, J. D., Tang, J., Huffman, L. C. (2004). Patterns of agreement between parent and child
ratings of emotional and behavioral problems in an outpatient clinical setting: When children endorse more problems.
Journal of Developmental and Behavioral Pediatrics, 25(3), 150–155.
Patenaude, A. F., & Kupst. M. (2005). Psychosocial functioning in pediatric cancer. Journal of Pediatric Psychology, 30(1), 9–27.
Price, J., Kassam-Adams, N., Alderfer, M. A., Christofferson, J., & Kazak, A. E. (2016). Systematic review: A reevaluation and update
of the integrative (trajectory) model of pediatric medical traumatic stress. Journal of Pediatric Psychology, 41(1), 86–97.
Pynoos, R., Rodriguez, N., Steinberg, A., Stuber, M., & Frederick, C. (1998). UCLA PTSD index for DSM-IV. Unpublished manuscript,
UCLA Trauma Psychiatry Service.
Varni, J. W., Burwinkle, T. M., Seid, M., & Skarr, D. (2003). The PedsQL 4.0 as a pediatric population health measure: Feasibility,
reliability, and validity. Ambulatory Pediatrics, 3(6), 329–341.
Weathers, F. W., Litz, B. T., Herman, D. S., Huska, J. A., & Keane, T. M. (1993). The PTSD Checklist (PCL): Reliability, validity, and
diagnostic utility. In Annual Convention of the International Society for Traumatic Stress Studies. San Antonio:
International Society for Traumatic Stress Studies.
Wijnberg‐Williams, B. J., Kamps, W. A., Klip, E. C., & Hoekstra‐Weebers, J. E. (2006). Psychological adjustment of parents of
pediatric cancer patients revisited: Five years later. Psycho‐Oncology, 15(1), 1–8.