This study examined predictors of borderline personality features in 30 youth diagnosed with bipolar disorder. Higher scores on a measure of borderline personality features were associated with increased self-injurious behaviors, impulsive aggression, and decreased family cohesion. These findings suggest that youth with bipolar disorder exhibiting these characteristics may be at increased risk of developing borderline personality disorder. Larger, longitudinal studies are still needed to validate these predictors. The study aims to help clinicians identify at-risk youth earlier to improve outcomes through targeted psychotherapy interventions.
Dr Sadgun Bhandari - A PRELIMNARY REVIEW. Dr. Sadgun Bhandari is a General Psychiatrist Consultant and an expert at the management of Serious Mental Illness especially Schizophrenia and Bipolar Affective Disorder.
Alex's Lemonade Stand Foundation holds an annual Childhood Cancer Symposium in Philadelphia. It is designed to be an educational resource, providing families with the opportunity to learn about issues and topics of treatment and beyond, while meeting other families in a group setting. Registration is free and is open to all those touched by childhood cancer, including patients and their siblings.
Presentation by: Melissa Alderfer, PhD.
Mary T. Rourke, Ph.D., discusses how medical traumatic stress impacts the whole family. This session is part of Alex's Lemonade Stand Foundation's annual Childhood Cancer Symposium. To listen to the audio recording please visit: http://www.alexslemonade.org/campaign/symposium-childhood-cancer.
Dr Sadgun Bhandari - A PRELIMNARY REVIEW. Dr. Sadgun Bhandari is a General Psychiatrist Consultant and an expert at the management of Serious Mental Illness especially Schizophrenia and Bipolar Affective Disorder.
Alex's Lemonade Stand Foundation holds an annual Childhood Cancer Symposium in Philadelphia. It is designed to be an educational resource, providing families with the opportunity to learn about issues and topics of treatment and beyond, while meeting other families in a group setting. Registration is free and is open to all those touched by childhood cancer, including patients and their siblings.
Presentation by: Melissa Alderfer, PhD.
Mary T. Rourke, Ph.D., discusses how medical traumatic stress impacts the whole family. This session is part of Alex's Lemonade Stand Foundation's annual Childhood Cancer Symposium. To listen to the audio recording please visit: http://www.alexslemonade.org/campaign/symposium-childhood-cancer.
Cognitive Behavioral Treatments for Anxietyin Children With WilheminaRossi174
Cognitive Behavioral Treatments for Anxiety
in Children With Autism Spectrum Disorder
A Randomized Clinical Trial
Jeffrey J. Wood, PhD; Philip C. Kendall, PhD; Karen S. Wood, PhD; Connor M. Kerns, PhD;
Michael Seltzer, PhD; Brent J. Small, PhD; Adam B. Lewin, PhD; Eric A. Storch, PhD
IMPORTANCE Anxiety is common among youth with autism spectrum disorder (ASD), often
interfering with adaptive functioning. Psychological therapies are commonly used to treat
school-aged youth with ASD; their efficacy has not been established.
OBJECTIVE To compare the relative efficacy of 2 cognitive behavioral therapy (CBT) programs
and treatment as usual (TAU) to assess treatment outcomes on maladaptive and interfering
anxiety in children with ASD. The secondary objectives were to assess treatment outcomes
on positive response, ASD symptom severity, and anxiety-associated adaptive functioning.
DESIGN, SETTING, AND PARTICIPANTS This randomized clinical trial began recruitment in
April 2014 at 3 universities in US cities. A volunteer sample of children (7-13 years) with ASD
and maladaptive and interfering anxiety was randomized to standard-of-practice CBT,
CBT adapted for ASD, or TAU. Independent evaluators were blinded to groupings. Data
were collected through January 2017 and analyzed from December 2018 to February 2019.
INTERVENTIONS The main features of standard-of-practice CBT were affect recognition,
reappraisal, modeling/rehearsal, in vivo exposure tasks, and reinforcement. The CBT
intervention adapted for ASD was similar but also addressed social communication and
self-regulation challenges with perspective-taking training and behavior-analytic techniques.
MAIN OUTCOMES AND MEASURES The primary outcome measure per a priori hypotheses was
the Pediatric Anxiety Rating Scale. Secondary outcomes included treatment response on the
Clinical Global Impressions–Improvement scale and checklist measures.
RESULTS Of 214 children initially enrolled, 167 were randomized, 145 completed treatment,
and 22 discontinued participation. Those who were not randomized failed to meet eligibility
criteria (eg, confirmed ASD). There was no significant difference in discontinuation rates
across conditions. Randomized children had a mean (SD) age of 9.9 (1.8) years; 34 were
female (20.5%). The CBT program adapted for ASD outperformed standard-of-practice CBT
(mean [SD] Pediatric Anxiety Rating Scale score, 2.13 [0.91] [95% CI, 1.91-2.36] vs 2.43 [0.70]
[95% CI, 2.25-2.62]; P = .04) and TAU (2.93 [0.59] [95% CI, 2.63-3.22]; P < .001). The CBT
adapted for ASD also outperformed standard-of-practice CBT and TAU on parent-reported
scales of internalizing symptoms (estimated group mean differences: adapted vs
standard-of-practice CBT, −0.097 [95% CI, −0.172 to −0.023], P = .01; adapted CBT vs TAU,
−0.126 [95% CI, −0.243 to −0.010]; P = .04), ASD-associated social-communication
symptoms (estimated group mean difference: adapted vs standard-of-practice CBT, −0.115
[95% CI, −0223 to −0 ...
11. Identifying the Elements of the Limitations & ImplicationsGo tBenitoSumpter862
11. Identifying the Elements of the Limitations & Implications
Go to the Limitations/Implications section(s) and identify the limitations of the study and how those limitations impacted the whole study.
12. Identifying the Elements of the Conclusion Section
Go to the Conclusion section and identify the conclusive statements of the study and the recommendations made for future research.
POST # 1 EDITHA
When assessing an adolescent with bipolar disorder, what are some of the diagnostic and treatment challenges the clinician might face?
Bipolar disorder is a serious mental health disorder that is often first diagnosed during young adulthood or adolescence. Symptoms of the illness, however, also can appear in early childhood. Although once thought rare in children, diagnosis of bipolar disorder in children has significantly increased over the last decade (Papolos & Bronsteen, 2018). Despite the increased diagnosis of bipolar disorder in children, assessment and diagnosis remain challenging and controversial. This is, in part, because of the lack of research on this disorder in children and adolescents and the growing recognition that the disease can present differently in children from how it presents in adults (AACAP, 2019). Over the years, more attention has focused on the unique presentation of bipolar disorder in the young that has introduced new ways of looking at this disease and assessing it in children.
The importance of identifying the presence of bipolar disease at an early age is highlighted by data showing that adults in whom bipolar disease started at an early age have a more severe course of the illness compared with adult-onset disease. Early-onset disease is associated with a higher risk of suicide; severe mood lability and polarity; lower quality of life and greater functional impairment; higher rates of comorbidity; and a higher risk of substance use disorders compared with adult-onset disease (Papolos & Bronsteen, 2018). Although some children meet the criteria established for adults categorized in the DSM-5, many children fall outside these classical categories, and diagnosis in these children is particularly challenging and difficult (APA, 2013). For these children, additional information beyond what is provided in the DSM may help make an accurate diagnosis which causes increased challenges in assessment and diagnosis.
References
Papolos, D, & Bronsteen A. (2018) bipolar disorder in children: assessment in general pediatric practice. Curr Opin Pediatr, 25(3):419-426.
American Academy of Child and Adolescent Psychiatry (AACAP). (2019) bipolar disorder: Parents’ Medication Guide for Bipolar Disorder in Children & Adolescents.
American Psychiatric Association (APA) (2013). Diagnostic and Statistical Manual of Mental Disorders, Fifth Edition (DSM-5). Washington, DC: American Psychiatric Association.
RESEARCH ARTICLE
Association of suicidal behavior with exposure
to suicide and suicide attempt: A systematic
...
11. Identifying the Elements of the Limitations & ImplicationsGo tSantosConleyha
11. Identifying the Elements of the Limitations & Implications
Go to the Limitations/Implications section(s) and identify the limitations of the study and how those limitations impacted the whole study.
12. Identifying the Elements of the Conclusion Section
Go to the Conclusion section and identify the conclusive statements of the study and the recommendations made for future research.
POST # 1 EDITHA
When assessing an adolescent with bipolar disorder, what are some of the diagnostic and treatment challenges the clinician might face?
Bipolar disorder is a serious mental health disorder that is often first diagnosed during young adulthood or adolescence. Symptoms of the illness, however, also can appear in early childhood. Although once thought rare in children, diagnosis of bipolar disorder in children has significantly increased over the last decade (Papolos & Bronsteen, 2018). Despite the increased diagnosis of bipolar disorder in children, assessment and diagnosis remain challenging and controversial. This is, in part, because of the lack of research on this disorder in children and adolescents and the growing recognition that the disease can present differently in children from how it presents in adults (AACAP, 2019). Over the years, more attention has focused on the unique presentation of bipolar disorder in the young that has introduced new ways of looking at this disease and assessing it in children.
The importance of identifying the presence of bipolar disease at an early age is highlighted by data showing that adults in whom bipolar disease started at an early age have a more severe course of the illness compared with adult-onset disease. Early-onset disease is associated with a higher risk of suicide; severe mood lability and polarity; lower quality of life and greater functional impairment; higher rates of comorbidity; and a higher risk of substance use disorders compared with adult-onset disease (Papolos & Bronsteen, 2018). Although some children meet the criteria established for adults categorized in the DSM-5, many children fall outside these classical categories, and diagnosis in these children is particularly challenging and difficult (APA, 2013). For these children, additional information beyond what is provided in the DSM may help make an accurate diagnosis which causes increased challenges in assessment and diagnosis.
References
Papolos, D, & Bronsteen A. (2018) bipolar disorder in children: assessment in general pediatric practice. Curr Opin Pediatr, 25(3):419-426.
American Academy of Child and Adolescent Psychiatry (AACAP). (2019) bipolar disorder: Parents’ Medication Guide for Bipolar Disorder in Children & Adolescents.
American Psychiatric Association (APA) (2013). Diagnostic and Statistical Manual of Mental Disorders, Fifth Edition (DSM-5). Washington, DC: American Psychiatric Association.
RESEARCH ARTICLE
Association of suicidal behavior with exposure
to suicide and suicide attempt: A systematic
...
BRIEF REPORTScreening for Depression Among Minority Young VannaSchrader3
BRIEF REPORT
Screening for Depression Among Minority Young Males Attending a
Family Planning Clinic
Ruth S. Buzi and Peggy B. Smith
Baylor College of Medicine
Maxine L. Weinman
University of Houston
The Center for Epidemiologic Studies Depression Scale (CES-D) was used to assess depression among
535 African American and Hispanic young males ages 14 to 27 attending a family planning clinic. The
assessment indicated that 119 (22.2%) males met criteria for depression. The study also examined the
associations between depression, sociodemographics, and service requests. Depressed males were more
likely than nondepressed males to be Hispanic and to request services related to relationships, feelings,
financial resources, physical issues, and well-being. The findings indicated that young males who are
affected by depression have unmet needs, but when given an opportunity, are able to express those needs.
Because family planning clinics are increasing the number of male clients, they are well positioned to
screen them for depression.
Keywords: young males, depression, request for services
Major Depressive Disorder (MDD) is recognized as one of
the most common chronic conditions today. According to the
U.S. Department of Health and Human Services (2012), ap-
proximately 2 million adolescents, or 8.0% of the population
ages 12 to 17, had at least one major depressive episode during
2010. A recent report by the Substance Abuse and Mental
Health Services Administration (SAMHSA, 2012) indicates
that one in five American adults aged 18 or older, or 45.6
million, people had mental illness in the past year. The rate of
mental illness was twice as high among those 18 –25 (29.8%)
than among those aged 50 and older (14.3%).
Males experience more persistent depressive symptoms and
disorders from adolescence into adulthood than females (Dunn
& Goodyer, 2006; Colman, Wadsworth, Croudace, & Jones,
2007). Non-Hispanic African American males tend to have the
highest rates of MDD at 13.2%, followed by Hispanics or
Latinos (12.7%) and then non-Hispanic Whites (8.7%) U.S.
Department of Health & Human Services, 2012). Depression
among minority adolescents and young adults was found to be
related to stress, lack of social resources, and low socioeco-
nomic status (Brown, Meadows, & Elder, 2007). Risk factors
for African American men’s depression include economic
strain, interpersonal conflicts, and racial discrimination (Wat-
kins, Green, Rivers, & Rowell, 2006). Hispanic and African
American males also display significantly earlier onset of MDD
compared with their White counterparts (Riolo, Nguyen, Gre-
den, & King, 2005).
Despite the fact that males also suffer from depression, they
seek mental help from health care professionals less frequently
than females, which only further decreases the likelihood of
diagnosing their mental health disorders (Addis & Mahalik,
2003; Smith, Braunack-Mayer, & Wittert, 2006). Males often
feel pressured to avoid emotional expres ...
BRIEF REPORTScreening for Depression Among Minority Young .docxjackiewalcutt
BRIEF REPORT
Screening for Depression Among Minority Young Males Attending a
Family Planning Clinic
Ruth S. Buzi and Peggy B. Smith
Baylor College of Medicine
Maxine L. Weinman
University of Houston
The Center for Epidemiologic Studies Depression Scale (CES-D) was used to assess depression among
535 African American and Hispanic young males ages 14 to 27 attending a family planning clinic. The
assessment indicated that 119 (22.2%) males met criteria for depression. The study also examined the
associations between depression, sociodemographics, and service requests. Depressed males were more
likely than nondepressed males to be Hispanic and to request services related to relationships, feelings,
financial resources, physical issues, and well-being. The findings indicated that young males who are
affected by depression have unmet needs, but when given an opportunity, are able to express those needs.
Because family planning clinics are increasing the number of male clients, they are well positioned to
screen them for depression.
Keywords: young males, depression, request for services
Major Depressive Disorder (MDD) is recognized as one of
the most common chronic conditions today. According to the
U.S. Department of Health and Human Services (2012), ap-
proximately 2 million adolescents, or 8.0% of the population
ages 12 to 17, had at least one major depressive episode during
2010. A recent report by the Substance Abuse and Mental
Health Services Administration (SAMHSA, 2012) indicates
that one in five American adults aged 18 or older, or 45.6
million, people had mental illness in the past year. The rate of
mental illness was twice as high among those 18 –25 (29.8%)
than among those aged 50 and older (14.3%).
Males experience more persistent depressive symptoms and
disorders from adolescence into adulthood than females (Dunn
& Goodyer, 2006; Colman, Wadsworth, Croudace, & Jones,
2007). Non-Hispanic African American males tend to have the
highest rates of MDD at 13.2%, followed by Hispanics or
Latinos (12.7%) and then non-Hispanic Whites (8.7%) U.S.
Department of Health & Human Services, 2012). Depression
among minority adolescents and young adults was found to be
related to stress, lack of social resources, and low socioeco-
nomic status (Brown, Meadows, & Elder, 2007). Risk factors
for African American men’s depression include economic
strain, interpersonal conflicts, and racial discrimination (Wat-
kins, Green, Rivers, & Rowell, 2006). Hispanic and African
American males also display significantly earlier onset of MDD
compared with their White counterparts (Riolo, Nguyen, Gre-
den, & King, 2005).
Despite the fact that males also suffer from depression, they
seek mental help from health care professionals less frequently
than females, which only further decreases the likelihood of
diagnosing their mental health disorders (Addis & Mahalik,
2003; Smith, Braunack-Mayer, & Wittert, 2006). Males often
feel pressured to avoid emotional expres.
1. R.S. Kahlon, MD1,2, C.D. Verrico, PhD1,3, A. Shah, MD1,2, B.A. Syed, MD1,2, P.A. Amin, MD1,2,T. Vu-Sowers, MD1,2, K.P. Taslimi, PhD4, R.P. Arvind, MD1,2, L.E. Wood, LCSW2, C. Sharp, PhD1,5,6, U.
Ramamurthy, MBA, MS PhD4, X. Lu, MS4, O.O. Okusaga, MD, MScPHR7, L.L. Williams, DO1,2, K. Saxena, MD1,2
1Menninger Department of Psychiatry and Behavioral Sciences, Houston, TX, 2Psychiatry Service, Texas Children’s Hospital, Houston, TX, 3Department of Psychiatry, Michael E. DeBakey V.A. Medical Center, Houston, TX, 4 Psychology Section, Department of
Pediatrics, Texas Children’s Hospital, Houston, TX, 5The Menninger Clinic, Houston, TX, 6Department of Psychology, University of Houston, Houston, TX, 7UT Harris County Psychiatric Center, Houston, TX
Self-Injurious Behavior, Impulsive Aggression and Decreased Family Cohesion in
Bipolar Youth: Probable Determinants of Emerging Borderline Personality.
Objectives
• Borderline Personality Disorder (BPD)
and adult Bipolar Disorder (BD) are often
diagnosed as comorbid disorders in
adults and adolescents 1,2.
• These disorders furthermore share
common correlates and risk factors3.
• This study aims to examine the
predictors that may increase the
likelihood of borderline features in youth
with BD.
Conclusions
• The study results demonstrate that
higher BPFS scores are observed in youth
with BD, who exhibit increased self-
injurious behaviors, increased impulsive
aggression, and decreased family
cohesion.
• The significance of these findings lies in
assisting clinicians in recognizing youth
with BD, who may be on the trajectory of
developing BPD.
• This in turn, can aid clinicians in
implementing specific psychotherapeutic
interventions which might improve
outcomes. Further research examining
longitudinal data with larger samples is
needed to validate these findings.
.
Materials and Methods
• 30 participants (M:16, F:14), aged 7–17
years, inclusive (Mean Age 12.95 ± 3.08
years) were recruited in an outpatient
specialty mood disorders clinic.
• Participants met DSM-IV-TR criteria for
BD I (n=19) and BD II (n=3). Also, the
Course and Outcome of Bipolar Youth
(COBY) criteria was used to establish the
BD–Not Otherwise Specified diagnosis
(n=7).
References
Results
• Significant positive associations were seen
between total score of BPFS Child Version
and:
- Total score of the Buss Perry Aggression
Questionnaire (BPAQ) (β=0.35, p<0.01)
- All the individual subscale scores of
BPAQ.
• The Self-harm subscale of BPFS Child
Version showed a significant and positive
association with
-Total score of the BPAQ (β=0.12, p<0.01)
-All the individual subscale scores of
BPAQ.
• Perceived Family cohesion scores were
negatively associated with
- Total score (β=-0.21, p<0.03)
-Self-Harm component (β=-0.69, p<0.05)
of the BPFS Parent Version.
Materials and Methods
• A battery of validated measures,
including the 24-item self-report
Borderline Personality Features Scale
(BPFS) was administered to obtain
cross-sectional data from study
participants and their primary
caregiver4.
• Multivariable linear regression
analyses examined associations
between BPFS (total and sub-scale)
scores and various psychopathology-
related predictor variables, while
adjusting for age, race, primary BD
diagnosis and the interval between
completion of the BPFS and other
predictor variables.
Table 1: Demographics CASES
N 30
Gender
N of males 16
N of females 14
Age in years (mean ± SD) 12.95 ± 3.08
Race
N of White or Caucasian 25
N of Black or African 4
N of Other 1
Ethnicity
Non-Hispanic or Non-latino 25
Hispanic or Latino 5
Diagnosis
Bipolar 1 20
Bipolar 2 3
COBY Bipolar NOS 7
Mean Age(±SD)
Bipolar 1 13.3 ± 2.80
Bipolar 2 14.8 ± 0.290
COBY Bipolar NOS 12.8 ± 3.76
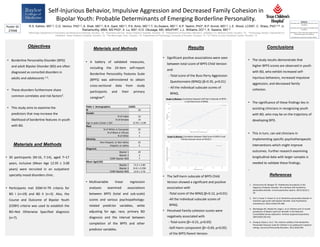
R² = 0.128
30
50
70
90
50 60 70 80 90 100 110
FACES-parent,FamilyCohesion
BPFS-parent, Score
R² = 0.5579
40
60
80
100
120
140
160
5 10 15 20 25 30 35
BPAQScore
BPFS-child, Self-Harm Subscale Score
Graph A (Below): Correlation between Self-Harm Subscale of BPFS-
C and Total Score of BPAQ
Graph B (Below): Correlation between Total Score of BPFS-P and
Family Cohesion Score of FACES II
1. Zimmerman M, Morgan TA. Problematic boundaries in the
diagnosis of bipolar disorder: the interface with borderline
personality disorder. Current psychiatry reports. 2013;15(12):1-
10.
2. Yen S, Frazier E, Hower H, et al. Borderline personality disorder in
transition age youth with bipolar disorder. Acta Psychiatrica
Scandinavica.2015;132(4):270-280.
3. Merikangas KR, Akiskal HS, Angst J, et al. Lifetime and 12-month
prevalence of bipolar spectrum disorder in the National
Comorbidity Survey replication. Archives of general psychiatry.
2007;64(5):543-552.
4. Chang B, Sharp C, Ha C. The criterion validity of the Borderline
Personality Features Scale for Children in an adolescent inpatient
setting. Journal of Personality Disorders. 2011;25(4):492.
Disclosures:
Kirti Saxena, MD : Grant Support from John S. Dunn
Foundation
Carla Sharp, PhD: Grant Support from McNair Family
Foundation
Christopher D. Verrico, PhD: Grant Support from The
United States Department of Defense
No Disclosures to report from any other authors.
Poster ID:
27048