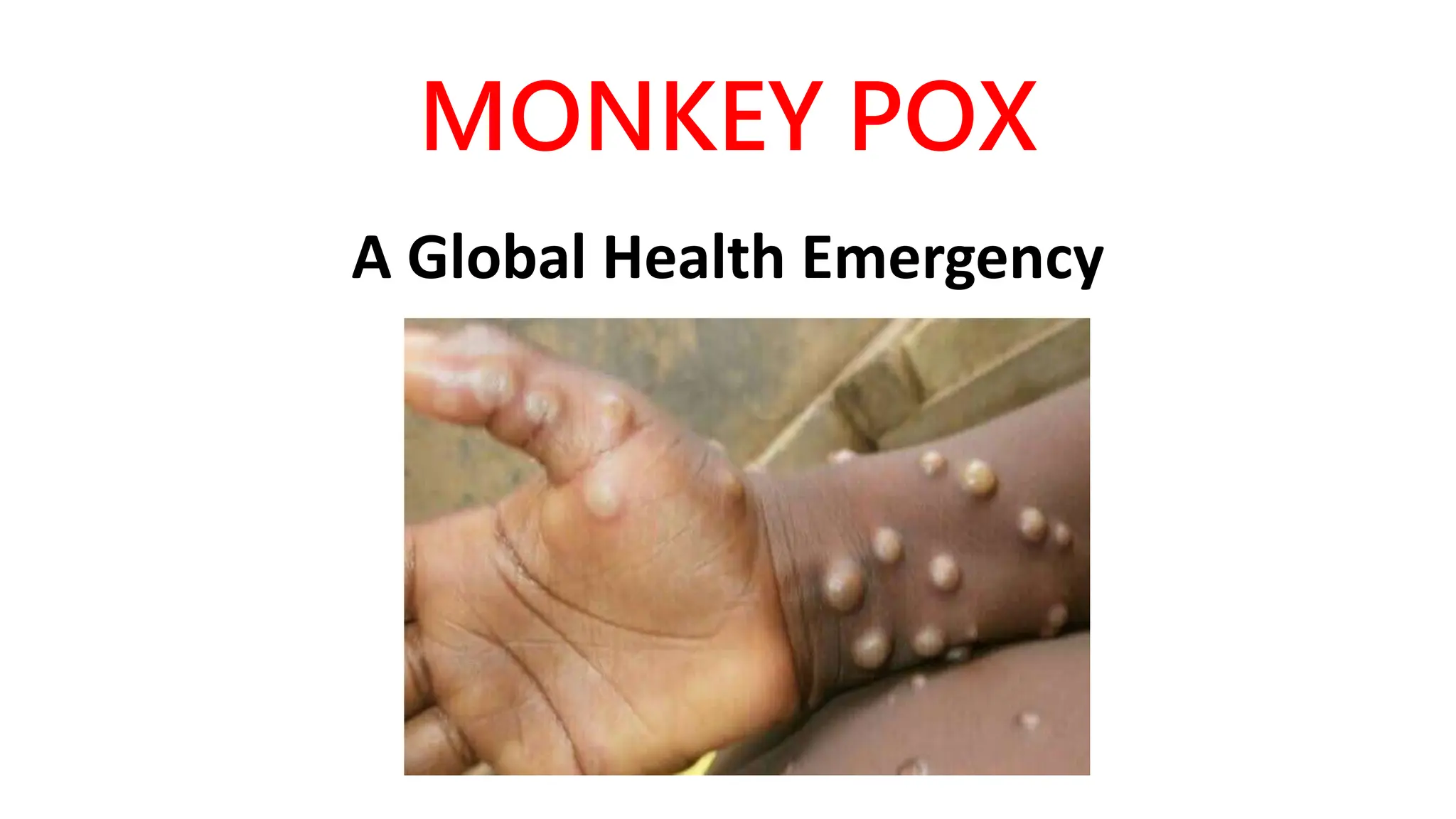
Monkeypox is a viral zoonosis that has emerged as a significant global health concern, particularly after the cessation of smallpox vaccination. The disease first identified in humans in 1970 has seen outbreaks in various countries, including a notable surge in the U.S. and India in 2022. The World Health Organization declared monkeypox a Public Health Emergency of International Concern on July 24, 2022, intensifying efforts for surveillance, treatment, and preventive measures against its spread.























































































![CTEV [ clubfoot] DR ARUN LAL ,DR MOHAMED ASHRAF travancore medical college k...](https://cdn.slidesharecdn.com/ss_thumbnails/ctevclubfootdrarunlaldrmohamedashraftravancoremedicalcollegekollamkeralaindia-260208063247-18fc466c-thumbnail.jpg?width=640&height=640&fit=bounds)