Downloaded 14 times


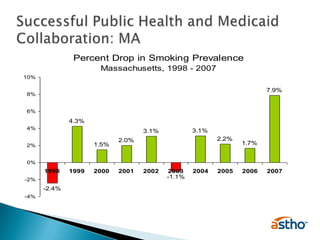
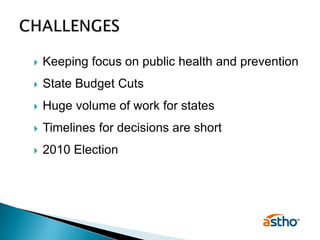




The document discusses the roles of state health agencies in enhancing efficiency within health systems, particularly in response to the Affordable Care Act. It highlights collaboration opportunities between public health and Medicaid, showcases successful initiatives like tobacco cessation programs in Massachusetts, and addresses challenges faced by health agencies, such as budget cuts. Ultimately, it advocates for the importance of public health investment and the need for strong partnerships among stakeholders to improve health outcomes.










































































































