Downloaded 359 times




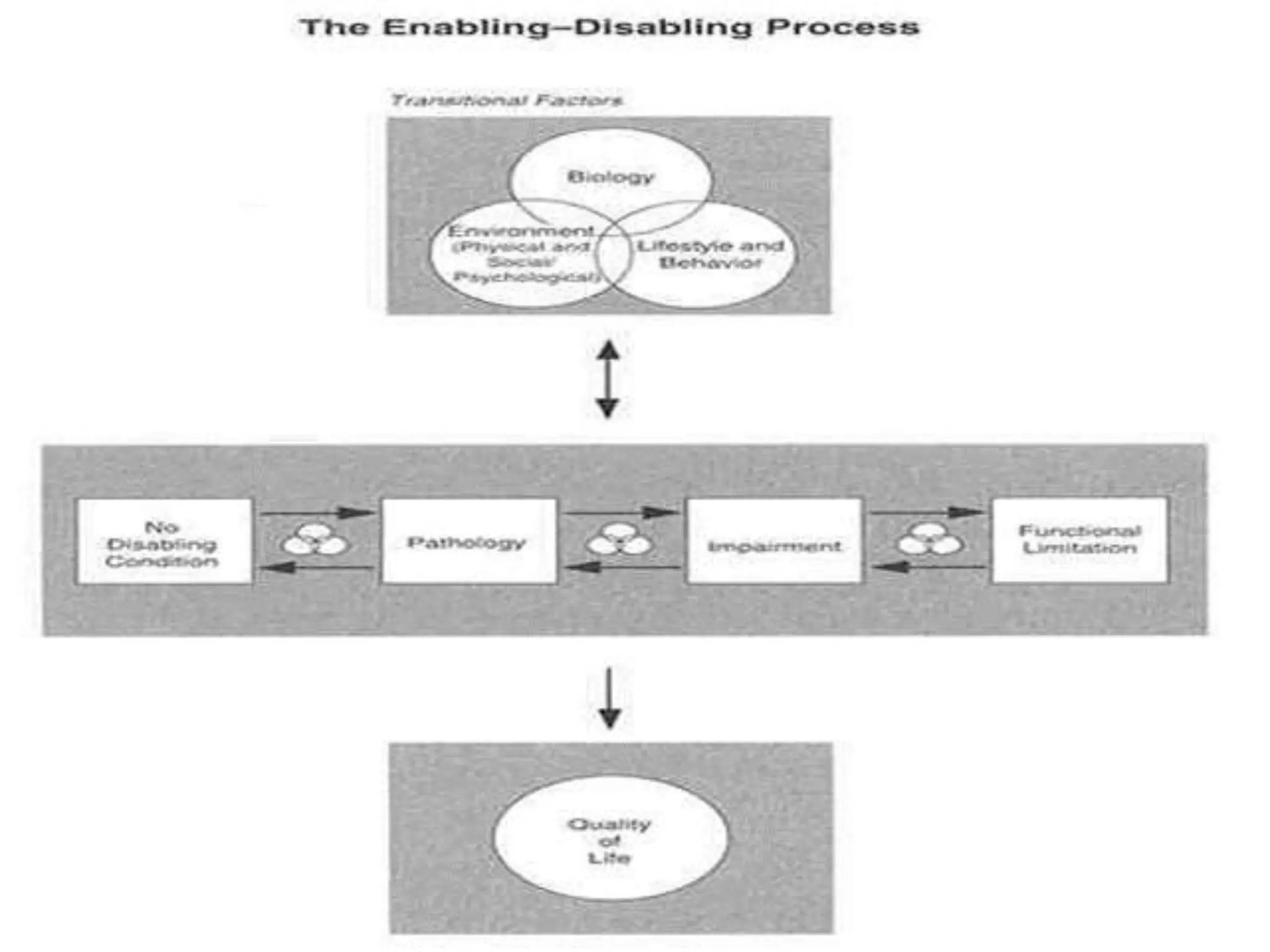

The document discusses models and methods of rehabilitation. It describes rehabilitation as helping a person reach their fullest potential physically, psychologically, socially, and educationally given their limitations. Rehabilitation nursing aims to restore abilities, prevent further disability, protect abilities, and assist patients. Principles of rehabilitation include beginning rehabilitation early, restoring independence, maximizing function within limits, and focusing on specific conditions. Methods include neurological, cardiac, drug, alcohol, physical, medical, vocational, vestibular, and stroke rehabilitation as well as community-based approaches. Models of rehabilitation include the Nagi, IOM, NCMRR, and new IOM models which define concepts like impairment, functional limitation, and disability and their interactions.