1. Mini- case (1) – Dementia and delirium
Dr Adam Feather – Lead for Medicine for the Elderly
2. Mini-case (1)
Mr Richard Lewis is a 79 year old retired train driver. He
is attending the outpatient clinic with his wife for the first
time.
The letter from his GP states that apart from
hypertension and benign prostatic hypertrophy (BPH),
for which he had a TURP some five years ago, he has
been very well and independent.
His wife brought him to the GP surgery at her ‘wits end’
saying she could no longer live with him and that ‘he
was driving her round the bend’. After a lengthy
consultation it seemed the main problem was Mr Lewis’
memory. The GP apologised for the rather ‘detail free’
letter but hoped you would be able to ascertain a better
history.
(1) What questions would you like to ask
regarding Mr Lewis’ memory problems?
3. Mini-case (1)
May need to take separate histories from patient and relative (with
permission). The Hx should be directed at (a) making / confirming a
diagnosis and (b) excluding reversible or treatable causes e.g.
depression, cerebral mets, B12 and folate deficiency,
hypothyroidism
HPC – Onset, progression and pattern of deterioration, things that
patient has noticed (insight), things that wife has noticed about
memory e.g. what he is finding difficult (ADLs); ‘Functionality’
Cardiovascular risk – IHD, Stroke, PVD, DM, Hypertension, Smoking,
alcohol excess, lipids
PH – Head injury, CNS disease, mental health
FH – dementia, Premature CV death
DH – Antiplatelets (CV protection), anti-psychotics
SH – occupation, education, social support, ADLs and function
ROS – general health (see above)
4. Mini-case (1)
Mrs Lewis explains that he has been slowly
deteriorating over the past 2 years and that it is
now ‘impossible to live with him’. He cannot
remember even simple things such as the way to
his bowls club, which is just around the corner from
their home.
The SpR examines Mr Lewis his BP = 160/90 but
otherwise general, CVS, RS, abdominal and
neurological examinations are all within normal
limits.
(2) Under the following headings think of a question or
test for the patient to perform to test their ‘memory’.
Long term memory
Short term memory
Language skills
Draw a shape
Concentration
Executive function
5. Folstein (MMSE)
Long term memory – Place – Country, Town,
Area, (Building)
Short term memory – 3 objects ( repeat, 5
minute)
Language skills - Write a sentence; follow 3
stage command
Draw a shape - intersecting pentagons
Concentration – serial 7s, WORLD / DLROW
Executive function – None!
Folstein MF, Folstein SE, McHugh PR; "Mini-mental state". A practical method for grading the
cognitive state of patients for the clinician. J Psychiatr Res. 1975 Nov;12(3):189-98.
6. Mini-case (1)
Mr Lewis scores 6 / 10 and 21 / 30 on the
AMTS and the MMSE respectively,
principally losing marks on short term
memory and orientation tests.
The SpR tells Mr and Mrs Lewis that she
will need to send Mr Lewis for several tests
including blood, radiology and a few
others.
(3) List the tests you would include in each
of the categories listed above, with a
reason or reasons for each.
7. Mini-case (1)
As with the history, investigations are directed at (a)
excluding contributing or treatable causes of cognitive
impairment and (b) confirming the diagnosis.
Bloods – FBC, U&Es, CBG, Lipids, ESR, TFTs, LFTs,
Calcium / magnesium, VDRL
Radiology – CXR and CT head scan
Others - ECG
8. Mini-case (1)
His investigations including FBC, U+Es, RBG,
LFTs, cCa, TFTs, ESR, VDRL, CXR and ECG are
relatively unremarkable other than some signs of
LVH on his ECG and cardiomegaly on his chest
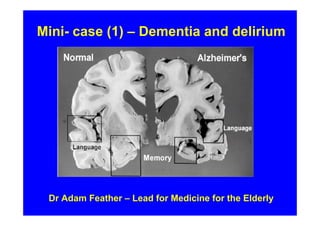
radiograph. The CT head scan shows ‘generalised
cerebral atrophy with no signs of SOL or previous
stroke disease’
(4) What is the most likely cause for the
signs of LVH on the ECG?
(5) What is the most likely cause for the
cerebral atrophy on the CT head scan?
11. Mini-case (1)
The SpR discusses the results with Mr and
Mrs Lewis and tells them he probably has
Alzheimer’s disease. She recommends he
starts on a ‘new medication’ which has been
shown to slow the deterioration of the
disease.
(6) List two possible ‘new medications’ with
their side effects.
(7) You may also need to add another
medication in view of his BP =160/90. List
another medication and its side effects. Do
these two medications interact?
12. Mini-case (1)
Drugs can only be prescribed by ‘expert’ – geriatrician, psychiatrist or neurologist with a
specialist interest (see NICE guidelines in BNF):
• Donepezil – reversible Acetylcholinstesterase inhibitor – SEs- GI – N&V, diarrhoea,
halucination, agitation, insomnia, Peptic ulcers (rare), SAN and AVN block
• Galantamine - reversible Acetylcholinstesterase inhibitor and some Nicotinic receptor
agonist effects; SEs – similar to Donepezil – also may induce IHD and Stroke,
hypokalaemia, V. rarely: GI bleed, parkinsonism, dysphagia
• Rivastigmine - reversible Acetylcholinstesterase inhibitor – similar side effect to above
including PUdx, parkisonism, bradycardia
• Memantine – N-Methyl-D-Aspartate (NMDA) – Receptor antagonist;Same group as
Ketamine. SEs – headache, hypertension, constipation, abnormal gait. Psychosis
including hallucination and suicidal ideation (very rare)
• Anti-hypertensives – A – C or D
Bendrofluomethiazide
ACEIs – Perindopril, Rampril, Lisinopril
A2RB – Losartan, Valsartan
Beta-blockers
Calcium channel blockers
Doxazosin
13. Mini-case (1)
The SpR discusses the home
circumstances with Mrs Lewis and
the current difficulties that she is
having.
(8) How would you help both Mr
and Mrs Lewis maintain Mr Lewis
at home?
14. Mini-case (1)
• Therapeutic interventions including
reducing CV risk
• Assessment of ADLs
• Assessment of home situation
• Dementia support; Respite – sitting
service, week(s) respite
• Day centre / Luncheon club
• Support for Mrs Lewis
15. Mini-case (1)
Three months later, Mrs Lewis is woken in the
middle of the night. She finds Mr Lewis getting
dressed, mumbling that he had forgotten to take
the dog for a walk. When she tells him that they
don’t have a dog and tries to get him to return to
bed, he becomes agitated and starts shouting.
Mrs Lewis cannot make sense of what he is
saying, and she feels frightened. She notices
that he has been incontinent of urine. She calls
the out-of-hours GP service, and an on-call GP
visits them at home.
(9) What is the diagnosis?
(10) What do you think the GP should do
when he reviews Mr Lewis, and why?
16. Mini-case (1)
• This is acute on chronic confusion = Delirium;
there are many many causes including
- Sepsis
- Metabolic
- Medications (inc withdrawal)
- Toxins – alcohol
- CNS – Causes of raised ICP; stroke; seizure
• The patient needs admission and further
investigation
17. Mini-case (1)
Mr Lewis is sent up to the ED for admission to
hospital. He is clerked in by the FY1 for Medicine for
the Elderly. On examination she finds tachycardia
(pulse rate 136bpm, poor volume and irregular) and
coarse crepitations in the left lung base. The FY1
organizes some investigations and arranges his
admission.
(9) What investigations would you order, and
why?
(10) What do you think are the most likely
diagnoses?
(11) What would be your management?
(12) Write up your management on the charts
provided.
18. Mini-case (1)
(9) Bloods – FBC, U&Es, RBG, LFTs, Blood
cultures x 2; ?CR(A)P,
Sputum – MC&S; Urinalysis
CXR, ECG, Venous or ABGs
CT head scan – if no improvement or focal
deficit
(10) Implied diagnoses – left lower lobe
pneumonia; Fast AF with resulting delirium
(11) Admit, CHEMO-IV (!) - Fluids, IV antibiotics,
sc heparin, IV digoxin or similar for Fast AF
21. Mini-case (1)
After a slow recovery the team feel that Mr Lewis
is ready for discharge. However whilst planning
for home Mrs Lewis and her daughter visit the
ward and tell the nurse in charge that they feel
Mr Lewis needs to go into a home as ‘they can
not manage him anymore’. When asked on the
consultant ward round the next day Mr Lewis is
insistent that he wants to go home. His MMSE is
21/30.
(13) How would you proceed?
22. Mini-case (1)
• Need to establish patient’s capacity – see
next slides
• If he retains capacity his wishes need to
be facilitated; however – the family will
need support, so a negotiation around his
level of care and support will need to take
place
• If no common ground / compromise can
be attained – a CPM will need to be held.
• Regardless Mr Lewis will need full MDT
assessment +/- home visit.
23. Mini-case (1)
(14) What do you understand by the
following terms?
(a) Mental capacity
(b) Enduring Power of Attorney
(EPA)
(c) Court of protection
24. Capacity
• Important changes were brought in around capacity by
the Mental Capacity Act (2005) – (see links at the end of
the presentation).
• All individuals are assumed to be mentally competent and
retain capacity until proven otherwise.
A person lacks capacity if they fail one of the following
criteria:
(a) understanding the information relevant to the decision
(b) retaining the information (even if only for a short
period)
(c) using or weighing that information
(d) communicating the decision (by any means)
• An unwise or irrational decision is not necessarily an
incompetent decision.
• Individuals who do not have an advocate, require
assessment through the IMCA service (Independent
mental capacity advocate).
25. Enduring Power of Attorney
• This is a legal process
• A competent Individual gives the legal right to
one or more individuals (= ‘attorneys’) to
manage their financial affairs including property
• Unlike an ordinary power of attorney, an EPA
remains effective even if the individual becomes
mentally incompetent at a later date.
• An EPA can NOT be put in place once a person
loses capacity
see: http://www.enduringpowerofattorney.co.uk/
26. The Court of Protection
The Court has the same powers, rights, privileges and authority
in relation to mental capacity matters as the High Court. It is a
superior court of record and is able to set precedents (set
examples to follow in future cases).
The Court of Protection has the powers to:
• decide whether a person has capacity to make a particular decision
for themselves;
• make declarations, decisions or orders on financial or welfare
matters affecting people who lack capacity to make such decisions;
• appoint deputies to make decisions for people lacking capacity to
make those decisions;
• decide whether an LPA or EPA is valid; and
• remove deputies or attorneys who fail to carry out their duties, and
• hear cases concerning objections to register an LPA or EPA and
make decisions about whether or not an LPA or EPA is valid.
See http://www.publicguardian.gov.uk/about/court-of-protection.htm
27. Mini-case (1)
•http://www.sign.ac.uk/pdf/sign86.pdf
BGS guidelines on the diagnosis and management of
patients with dementia
• http://www.nice.org.uk/CG042
The NICE guidelines for care of patients with dementia
http://www.dh.gov.uk/en/Publicationsandstatistics/Bulletins
/theweek/Chiefexecutivebulletin/DH_4108436
Summary of Mental Capacity Act (2005)
http://www.bgs.org.uk/Publications/Compendium/compend
_2-2.htm
BGS guidelines on capacity