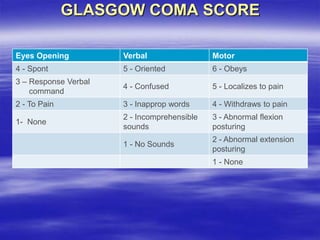
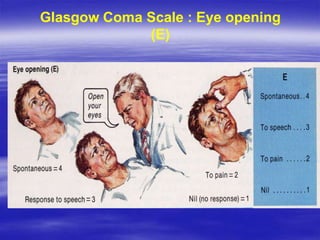
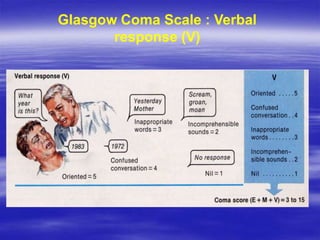
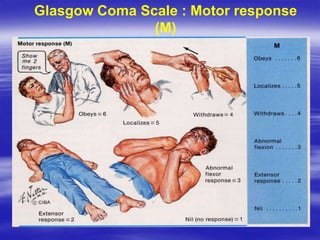
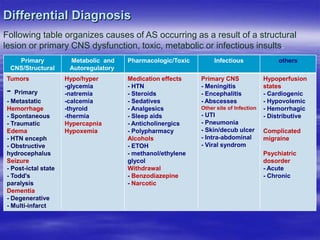
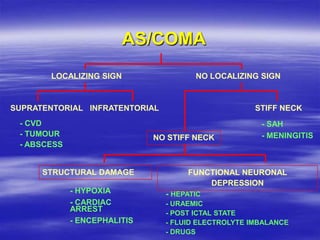
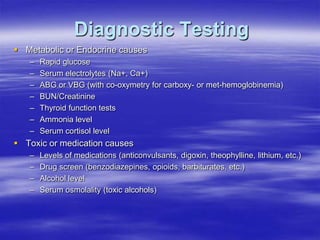
This document provides an overview of evaluating and managing a patient presenting with altered sensorium (AS). It defines sensorium and AS, noting that AS has many potential reversible and irreversible causes. The document outlines an approach including initial ABCDE assessment, detailed history, physical exam focusing on neurological assessment using Glasgow Coma Scale, and diagnostic testing to identify structural, metabolic, toxic, infectious, or other causes. Common differential diagnoses are listed. The goal is to recognize immediately life-threatening issues and rapidly reversible causes, and to systematically work through potential causes of AS.