Downloaded 18 times


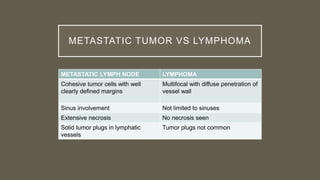
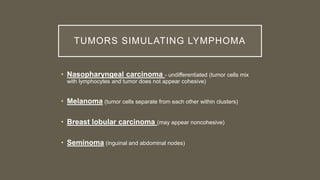
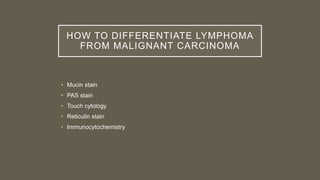
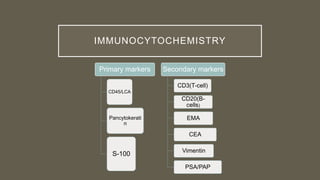
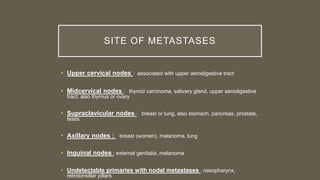



The document discusses metastasis to lymph nodes, focusing on its incidence, differentiation from lymphoma, and the significance of lymph node assessment for cancer staging. It highlights the TNM staging system and the role of lymph nodes in determining the extent of cancer, including various primary tumor sites and their association with lymphatic spread. Additionally, it describes methods to distinguish between lymphomas and malignant carcinomas using various staining techniques and immunocytochemistry.






































































![PERI-PROSTHETIC FRACTURE NAIL-PLATE CONSTRUCT [NPC].pptx](https://cdn.slidesharecdn.com/ss_thumbnails/drarunkumardrmohamedashrafperiprostheticfrasturenail-plateconstructnpc-260209164459-7e9d15a1-thumbnail.jpg?width=640&height=640&fit=bounds)



