Downloaded 151 times
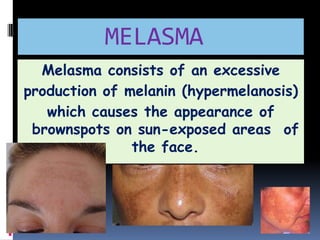
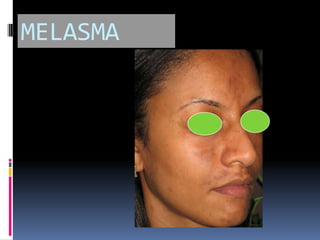

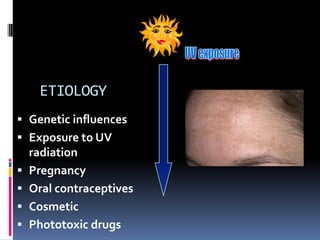
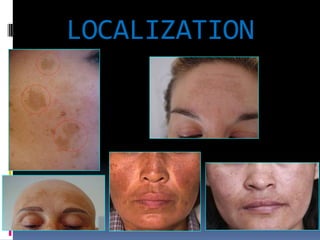


The document discusses melasma, a condition characterized by hypermelanosis resulting in brown spots on sun-exposed areas of the face, primarily affecting women of childbearing age. It highlights the epidemiology, classification, and pathophysiology of melasma, detailing its connection to genetic predisposition, UV radiation, and hormonal factors, particularly during pregnancy and contraceptive use. Additionally, it outlines the various clinical patterns, assessment methods such as the Melasma Area and Severity Index (MASI), and the role of vascular changes in the condition's pathogenesis.





















































![CTEV [ clubfoot] DR ARUN LAL ,DR MOHAMED ASHRAF travancore medical college k...](https://cdn.slidesharecdn.com/ss_thumbnails/ctevclubfootdrarunlaldrmohamedashraftravancoremedicalcollegekollamkeralaindia-260208063247-18fc466c-thumbnail.jpg?width=640&height=640&fit=bounds)












