Medicaid and Medicare at 50: Trends and Challenges
•
4 likes•7,314 views

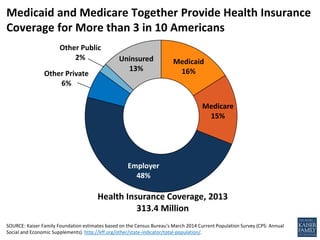
This document contains information about health insurance coverage in the United States in 2013. It shows that the largest sources of health insurance were employer-provided plans (48%), Medicaid (16%), Medicare (15%), and private plans (6%). It also notes that 13% of the population was uninsured. The document then discusses Medicaid and Medicare spending as part of the federal budget and shows these programs together account for nearly one-fourth of federal spending.

Recommended
Recommended
More Related Content
What's hot
What's hot (20)
Similar to Medicaid and Medicare at 50: Trends and Challenges
Similar to Medicaid and Medicare at 50: Trends and Challenges (20)
More from KFF
More from KFF (20)
Recently uploaded
Recently uploaded (20)
Medicaid and Medicare at 50: Trends and Challenges
- 1. Medicaid 16% Medicare 15% Employer 48% Other Private 6% Other Public 2% Uninsured 13% Health Insurance Coverage, 2013 313.4 Million SOURCE: Kaiser Family Foundation estimates based on the Census Bureau's March 2014 Current Population Survey (CPS: Annual Social and Economic Supplements). http://kff.org/other/state-indicator/total-population/. Medicaid and Medicare Together Provide Health Insurance Coverage for More than 3 in 10 Americans
- 2. Other Mandatory2 13% Discretionary Defense 17% Discretionary Non-Defense 17% Social Security 24% Medicare1 14% Medicaid 9%Net Interest 6% Actual FY 2014 Total Federal Outlays = $3.5 Trillion NOTE: FY is fiscal year. 1 Amount for Medicare is mandatory spending minus income from premiums and other offsetting receipts such as state contribution (clawback) payments to Medicare Part D). 2 ”Other” category includes other mandatory outlays (such as CHIP and Health Insurance Marketplace premium subsidies) minus income from offsetting receipts. SOURCE: Kaiser Family Foundation based on Congressional Budget Office, Budget and Economic Outlook Fiscal Years 2015-2025, January 2015. Medicare and Medicaid Comprise Nearly One-Fourth of Federal Spending
- 3. NOTE: FPL-- Federal Poverty Level. The FPL was $19,530 for a family of three in 2013. SOURCES: Kaiser Commission on Medicaid and the Uninsured (KCMU) and Urban Institute analysis of 2013 CPS/ASEC Supplement; Birth data - Maternal and Child Health Update, National Governors Association, 2012; Medicare data - Medicare Payment Advisory Commission, Data Book: Beneficiaries Dually Eligible for Medicare and Medicaid (January 2015), 2010 data; Functional Limitations - KCMU Analysis of 2012 NHIS data; Nonelderly with HIV - 2009 CDC MMP; Nursing Home Residents - 2012 OSCAR data. Medicaid’s Role for Selected Populations 1 in 5 Americans <65 1 in 3 children 2 in 3 nursing home residents
- 4. SOURCE: Kaiser Family Foundation analysis of the Medicare Current Beneficiary Survey 2010 Cost and Use file. Characteristics of the Medicare Population 1 in 2 Medicare Beneficiaries with incomes < $23,500 1 in 3 Medicare Beneficiaries with 5+ chronic conditions 1 in 4 Medicare Beneficiaries reporting fair/poor health status
- 5. 17% 17% 9% 30% 8% 22% 26% 22% 22% 28% 39% 43% 31% 52% 35% Total Health Services & Supplies $2,469 Billion Hospital Care $937 Billion Physicians $587 Billion Nursing Home Care $156 Billion Prescription Drugs $271 Billion Medicare Medicaid NOTE: Includes neither spending on CHIP nor administrative spending. Definition of nursing facility care was revised from previous years and no longer includes residential care facilities for mental retardation, mental health or substance abuse. The nursing facility category includes continuing care retirement communities. SOURCE: CMS, Office of the Actuary, National Health Statistics Group, National Health Expenditure Accounts, 2015. Data for 2013. Medicare and Medicaid Pay for Nearly 40% of Total Health Care Spending Nationwide
- 6. 3.40% 4.10% 4.80% Medicare Medicaid Private Insurance Projected Average Annual Increase in per capita spending, 2013-2023 SOURCE: Calculated based on data published in Projections (Table 17), National Health Expenditure Data. (Centers for Medicare & Medicaid Services, December 2013,) http://www.cms.gov/Research-Statistics-Data-and-Systems/Statistics-Trends-and- Reports/NationalHealthExpendData/NationalHealthAccountsHistorical.html . Medicare and Medicaid are Projected to Grow at Slower Rates than Private Insurance
- 7. $2,264 $2,402 $2,098 $948 $6,012 $2,845 $1,956 $2,074 $8,276 $5,247 $4,054 $3,023 Ages 85+ Ages 75-84 Ages 65-74 Under age 65 Premiums Services NOTE: Analysis excludes beneficiaries enrolled in Medicare Advantage plans. Premiums includes Medicare Parts A and B and other types of health insurance beneficiaries may have (Medigap, employer-sponsored insurance, and other public and private sources). SOURCE: Kaiser Family Foundation analysis of the Medicare Current Beneficiary Survey 2010 Cost and Use file. Affording the Rising Costs of Health Care Medicare Beneficiaries’ Out of Pocket Costs in 2010 for:
- 8. 18% 17% 15% 14% 13% 13% 13% 16% 19% 22% 23% 24% 25% 27% 28% 30% 31% 82% 83% 85% 86% 87% 87% 87% 84% 81% 78% 77% 76% 75% 73% 72% 70% 69% 1999 2000 2001 2002 2003 2004 2005 2006 2007 2008 2009 2010 2011 2012 2013 2014 2015 NOTE: Includes MSAs, cost plans, demonstration plans, and Special Needs Plans as well as other Medicare Advantage plans. SOURCE: Authors’ analysis of CMS Medicare Advantage enrollment files, 2008-2015, and MPR, “Tracking Medicare Health and Prescription Drug Plans Monthly Report,” 1999-2007; enrollment numbers from March of the respective year, with the exception of 2006, which is from April. The Increasing Role of Private Plans in Medicare Medicare Advantage Traditional Medicare Share of Medicare Beneficiaries Enrolled in Medicare Private Health Plans, 1999-2015
- 9. 39.7 47.7 64.4 81.8 89.2 92.8 0 10 20 30 40 50 60 70 80 90 100 2000 2010 2020 2030 2040 2050 Number of Medicare beneficiaries (in millions) SOURCE: Kaiser Family Foundation based on the 2014 Annual Report of the Boards of Trustees of the Federal Hospital Insurance and Federal Supplementary Medical Insurance Trust Funds. Financing Care for an Aging Population
- 10. TX 26% FL 18% NC 10% GA 8% Other States Not Moving Forward 39% Notes: Excludes legal immigrants who have been in the country for five years or less and immigrants who are undocumented. The poverty level for a family of three in 2015 is $20,090. Totals may not sum to 100% due to rounding. Source: “Number of Poor Uninsured Nonelderly Adults in the ACA Coverage Gap,” KFF State Health Facts. http://kff.org/health-reform/state-indicator/number-of-poor-uninsured-nonelderly-adults-in-the-aca-coverage-gap/#. Addressing the Coverage Gap in States that Have Not Expanded Medicaid 3.7 Million Uninsured Low-Income Share of Low-Income Uninsured Adults in the Coverage Gap By State:
- 11. SOURCE: Medicaid Managed Care Enrollment Reports, 2000-2011, CMS. The Increasing Role of Managed Care in Medicaid 38% 38% 39% 40% 41% 43% 44% 46% 47% 49% 2002 2003 2004 2005 2006 2007 2008 2009 2010 2011 Share of Medicaid Enrollment in comprehensive MCOs:
- 12. $3,985 $2,399 $3,234 $10,505 $4,091 $1,805 $64 $13 $6,137 $9,158 $5,790 $2,463 $3,247 $16,643 $13,249 Total Children Adults Individuals with Disabilities Elderly Per Enrollee Spending, FFY 2011 Acute Care Long-Term Care Source: Kaiser Commission on Medicaid and the Uninsured and Urban Institute estimates based on data from FY 2011 MSIS and CMS-64 reports. Because 2011 data were unavailable, 2010 data was used for Florida, Kansas, Maine, Maryland, Montana, New Mexico, New Jersey, Oklahoma, Texas, and Utah. Data for these 10 states were adjusted to 2010 spending levels. Meeting the Varied Needs of Populations Covered in Medicaid