A Snapshot of Cancer Spending and Outcomes
•
1 like•1,624 views

A Snapshot of Cancer Spending and Outcomes

Recommended
Recommended
More Related Content
What's hot
What's hot (20)
Similar to A Snapshot of Cancer Spending and Outcomes
Similar to A Snapshot of Cancer Spending and Outcomes (20)
More from KFF
More from KFF (20)
Recently uploaded
Recently uploaded (20)
A Snapshot of Cancer Spending and Outcomes
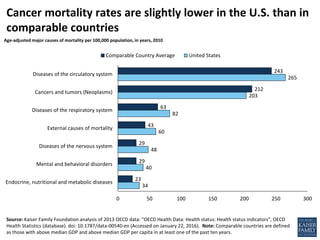
- 1. 34 40 48 60 82 203 265 23 29 29 43 63 212 243 0 50 100 150 200 250 300 Endocrine, nutritional and metabolic diseases Mental and behavioral disorders Diseases of the nervous system External causes of mortality Diseases of the respiratory system Cancers and tumors (Neoplasms) Diseases of the circulatory system Comparable Country Average United States Source: Kaiser Family Foundation analysis of 2013 OECD data: "OECD Health Data: Health status: Health status indicators", OECD Health Statistics (database). doi: 10.1787/data-00540-en (Accessed on January 22, 2016). Note: Comparable countries are defined as those with above median GDP and above median GDP per capita in at least one of the past ten years. Cancer mortality rates are slightly lower in the U.S. than in comparable countries Age-adjusted major causes of mortality per 100,000 population, in years, 2010
- 2. Source: Institute for Health Metrics and Evaluation. Global Burden of Disease Study Data Downloads, available here: http://ghdx.healthdata.org/global-burden-disease-study-2013-gbd-2013-data-downloads (Accessed May 11, 2016) Lung cancer is the largest contributor to disease burden among cancers for both males and females 133 143 145 167 170 183 220 364 366 980 - 400 800 1,200 Esophageal Brain and nervous system Liver Non-Hodgkin lymphoma Leukemia Other neoplasms Pancreatic Colon and rectal Prostate Lung and related MALES Age standardized disability adjusted life years (DALYs) rate per 100,000 population, males in the U.S., 2013 FEMALES Age standardized disability adjusted life years (DALYs) rate per 100,000 population, females in the U.S., 2013 86 91 97 102 151 158 164 249 517 639 - 500 1,000 Cervical Brain and nervous system Non-Hodgkin lymphoma Leukemia Other neoplasms Pancreatic Ovarian Colon and rectal Breast Lung and related
- 3. Source: Bureau of Economic Analysis Health Care Satellite Account (Blended Account) and National Health Expenditure Data Note: Spending on dental services, nursing homes, and prescriptions that cannot be allocated to a specific disease not included above. Data last updated January 25, 2016. Cancer spending accounts for about 7% of disease-based health expenditures Total expenditures in US $ billions by disease category, 2012 Ill-defined conditions, $247 Circulatory, $243 Musculoskeletal, $188 Respiratory, $158 Endocrine - $138 Nervous system - $133Cancers - $124 Injury - $118 Genitourinary - $113 Digestive - $107 Mental Illness - $80 Infectious diseases - $67 Dermatological - $44 Pregnancy, birth - $39 Other - $93
- 4. Source: Kaiser Family Foundation analysis of Bureau of Economic Analysis Health Care Satellite Account (Blended Account) Note: Expenditures on nursing home and dental care are not included in health services spending by disease. Data last updated January 25, 2016. While Cancer is one of the top contributors to disease burden, it was not a leading driver of medical services spending growth from 2000-2012 Contribution to medical services expenditure growth, by disease, 2000-2012 1.7% 2.3% 4.1% 4.4% 5.1% 5.3% 5.9% 6.2% 6.3% 6.5% 7.4% 8.5% 8.6% 11.0% 16.6% 0% 2% 4% 6% 8% 10% 12% 14% 16% 18% Pregnancy/childbirth Dermatological Mental illness Infectious diseases Digestive Injury and poisoning Genitourinary Other Cancer Respiratory Nervous system Endocrine Circulatory Musculoskeletal Ill-defined conditions
- 5. Source: Kaiser Family Foundation analysis of Bureau of Economic Analysis Health Care Satellite Account (Blended Account) Note: Expenditures on nursing home and dental care are not included in health services spending by disease. Data last updated January 25, 2016. Average growth in per capita spending for cancer was slightly lower than the average for all disease categories Average annual growth in expenditures by disease category (per capita), price index by disease category (cost to treat each case), and real expenditures by disease category (number of treated cases), 2000 - 2012 5.0% 4.6% 1.3% 5.4% 4.4% 1.9% 0.0% 1.0% 2.0% 3.0% 4.0% 5.0% 6.0% Spending per capita Cost to treat each case Number of treated cases Cancer All diseases
- 6. Source: Express Scripts 2015 Drug Trend Report Cancer medications were among the top 3 conditions for specialty drug spending in 2015 Express Scripts per-member-per-year spending, top 10 specialty therapy class drugs, 2015 $4.57 $5.79 $5.85 $6.64 $7.12 $31.53 $38.44 $49.62 $53.31 $89.10 $0 $10 $20 $30 $40 $50 $60 $70 $80 $90 $100 Sleep disorders Hemophilia Pulmonary hypertension Cystic fibrosis Growth Deficiency HIV Hepatitis C Oncology Multiple Sclerosis Inflammatory conditions