Download to read offline
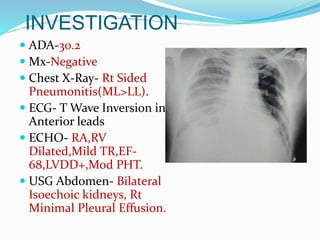
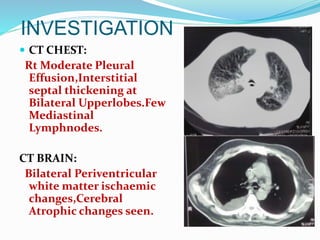
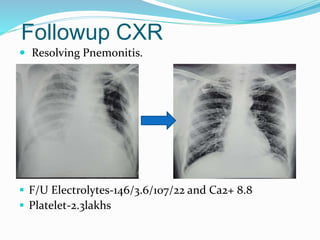
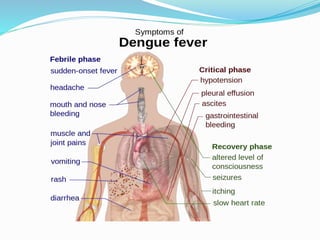


This document describes the case of a 70-year-old diabetic and hypertensive male who presented with fever, difficulty breathing, and drowsiness. Clinical examination found signs of pneumonia and sepsis. Investigations revealed dengue infection (positive IgM, IgG, NS1), metabolic encephalopathy, and hemorrhagic pleural effusion. The patient was diagnosed with dengue with acute lung injury and pneumonia. He received IV antibiotics, fluids, bronchodilators and supportive care. His condition improved with resolution of pneumonia seen on follow up imaging. The document then discusses dengue infection, its types and manifestations, diagnostic evaluation, and management including fluid resuscitation and symptomatic treatment.



































































