INTRODUCTION
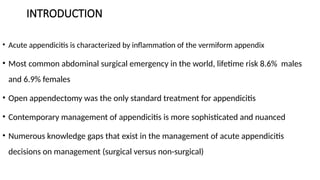
• Acute appendicitisis characterized by inflammation of the vermiform appendix
• Most common abdominal surgical emergency in the world, lifetime risk 8.6% males
and 6.9% females
• Open appendectomy was the only standard treatment for appendicitis
• Contemporary management of appendicitis is more sophisticated and nuanced
• Numerous knowledge gaps that exist in the management of acute appendicitis
decisions on management (surgical versus non-surgical)
DIAGNOSIS OF APPENDICITIS
•Accurate diagnosis is crucial to prevent complications, increases mortality from <0.1%
(uncomplicated) to ~5% (perforated)
• Key Diagnostic Tools:
• Clinical Scoring Systems: help stratify risk but lack universal adoption
• Imaging:
• Ultrasound (US): First-line in children and pregnant women (low cost, no radiation)
• CT Scan: Gold standard for adults (sensitivity >95%)
• MRI: Preferred in pregnancy when US is inconclusive
6.
CLASSIFICATION OF APPENDICITIS
•UNCOMPLICATED : localized appendicitis/non perforated
• COMPLICATED : perforated/abscess/mass
• Type:
• Acute - Marked by severe intolerable abdominal pain, worsens very quickly, usually
in hrs.
• Subacute - Recurrent but mild abdominal pain which starts on its own.
• Chronic - Clinically characterized by prolonged (>7/7) right lower quadrant pain
that may be intermittent and a normal WBC.
7.
EMERGENCY DEPARTMENT CARE
•NPO
• Intravenous (IV) access
• Administer crystalloid therapy to patients with clinical signs of dehydration or
septicemia-SMART trial
• Administer parenteral analgesic- acetaminophen/ NSAID/Opioid
• Antiemetic as needed for patient comfort
• Intravenous antibiotics- Broad-spectrum gram-negative and anaerobic coverage
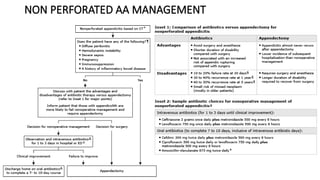
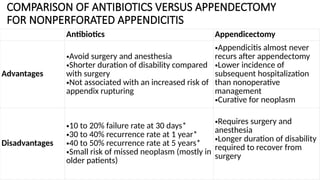
COMPARISON OF ANTIBIOTICSVERSUS APPENDECTOMY
FOR NONPERFORATED APPENDICITIS
Antibiotics Appendicectomy
Advantages
•Avoid surgery and anesthesia
•Shorter duration of disability compared
with surgery
•Not associated with an increased risk of
appendix rupturing
•Appendicitis almost never
recurs after appendectomy
•Lower incidence of
subsequent hospitalization
than nonoperative
management
•Curative for neoplasm
Disadvantages
•10 to 20% failure rate at 30 days*
•30 to 40% recurrence rate at 1 year*
•40 to 50% recurrence rate at 5 years*
•Small risk of missed neoplasm (mostly in
older patients)
•Requires surgery and
anesthesia
•Longer duration of disability
required to recover from
surgery
10.
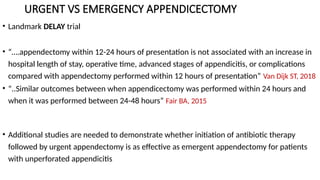
URGENT VS EMERGENCYAPPENDICECTOMY
• Landmark DELAY trial
• “….appendectomy within 12-24 hours of presentation is not associated with an increase in
hospital length of stay, operative time, advanced stages of appendicitis, or complications
compared with appendectomy performed within 12 hours of presentation” Van Dijk ST, 2018
• “..Similar outcomes between when appendicectomy was performed within 24 hours and
when it was performed between 24-48 hours” Fair BA, 2015
• Additional studies are needed to demonstrate whether initiation of antibiotic therapy
followed by urgent appendectomy is as effective as emergent appendectomy for patients
with unperforated appendicitis
11.
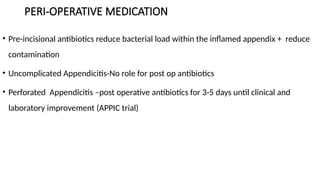
PERI-OPERATIVE MEDICATION
• Pre-incisionalantibiotics reduce bacterial load within the inflamed appendix + reduce
contamination
• Uncomplicated Appendicitis-No role for post op antibiotics
• Perforated Appendicitis –post operative antibiotics for 3-5 days until clinical and
laboratory improvement (APPIC trial)
12.
PATIENTS ON ANTIPLATELETOR ANTITHROMBOTIC
THERAPY
• Aspirin/CLOPIDOGREL
• Direct oral anticoagulants (DOACS)
• Warfarin
13.
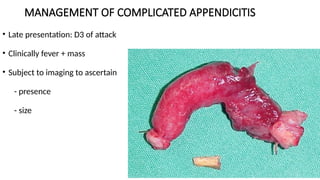
MANAGEMENT OF COMPLICATEDAPPENDICITIS
• Late presentation: D3 of attack
• Clinically fever + mass
• Subject to imaging to ascertain
- presence
- size
14.
PERFORATED ACUTE APPENDICITISAT UTH
• Prospective study of Perf AA at UTH-Samuel Phiri 2012
• Outcomes : 71 appendicectomies
: Perf rate 43.6%, 3-5 days
: M/F 2.5:1, Age peak 30-40 yrs
: 64.5% generalized peritonitis –Midline incision
: Mortality 1.4%
Factors contributing: pre Hosp pt delay, use of traditional meds (11%)
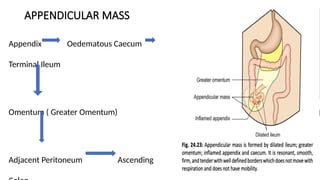
MANAGEMENT OF APPENDICULARMASS
Appendicular Lump- Don’t Operate (??)
• Severe adhesion/ Difficult to separate the part
• Bloody and dangerous to operate
• Risk of Faecal fistula
• Risk of iatrogenic injury
18.
OCHSNER- SHERREN REGIMEN
•NPO & IV Fluid supplements
• Antibiotics, Analgesics
• Temp, Pulse( 4 hourly) & Fluid record charting
• Allow oral liquid on subsequent days
• If more vomiting- antiemetic &/+ PPI
• If size of the lump decreases – continue the same
• After 6-8 weeks = Interval Appendectomy (current literature does not support this
view)
19.
MANAGEMENT OF APPENDICULARMASS
• Criteria for stopping conservative management
- Rising pulse/Temp
- Increasing/spreading abdominal pain
- Increase in size of mass
- Vomiting or copious gastric aspirate
• Failure of mass to resolve should raise suspicion of Ca or Crohn’s disease
• App 90% resolve with the OS regimen without incident
SURGICAL MANAGEMENT
• OpenAppendectomy (OA):
- Reserved for cases with dense adhesions or generalized peritonitis
• Timing of Surgery:
- Uncomplicated: Surgery within 12–24 hours is safe; delays >48 hours increase
complications
LAPAROSCOPIC APPENDICECTOMY
• SuitableIndications
• Uncomplicated appendicitis
• Appendicitis in pediatric patients
• Suspected appendicitis in pregnant women
• Preferred option for :
• Perforated appendicitis
• Appendicitis in elderly patients
• Appendicitis in obese patients
25.
LAPAROSCOPIC APPENDICECTOMY
• Advantages:
• increased cosmetic satisfaction
• decrease in the postoperative wound-infection rate
• shortens the hospital stay
• Mimimal pain
• Disadvantages:
• increased cost
• Longer operating time approximately 20 minutes longer than that of an open
appendicectomy
26.
DRAIN PLACEMENT
• Ingeneral, the use of abdominal drains is based on personal experience rather than
strict evidence-based guidelines, as exemplified by the surgical truism, “When in
doubt, drain,” first coined by Tait in 1905
• Surgical drains disadvantages: drain blockage, hindrance in the healing process,
prolonged hospital stay, and increased healthcare expenses
• Complications: erosion into abdominal viscera, fistula, entrapment, displacement,
kinking, or migration
• Increase the risk of enterocutaneous fistulas (4.2–7.5%) and wound infections (43–
85%), IO, Ileus
• Recent data have cast doubt on its efficacy in preventing postoperative complications
27.
COMPLICATIONS AND THEIRMANAGEMENT
• Wound Infections ( 20%):
̴ reduced with pre-op antibiotics
• Intra-abdominal Abscess (9–20%): Managed with drainage + antibiotics
• Paralytic Ileus: Avoid routine drain placement (increases fistula risk)
• Fecal fistula
• Stump Appendicitis: Rare but possible if residual tissue remains
• Bleeding/Iatrogenic Injury: More common in laparoscopic cases
• Appendicular tumor : < 2cm appendicectomy, > 2cm hemicolectomy
• Right inguinal hernia(direct)—due to injury to ilioinguinal nerve
• Respiratory problems and DVT
28.
CONTROVERSIES AND FUTUREDIRECTIONS
• Interval Appendectomy (IA):
- Debated necessity; some advocate for IA to rule out neoplasms (28% vs. 1% in
immediate surgery) -FINNISH trial
• Colonoscopy : all Patients above 40/not necessary
• Emerging Techniques: Endoscopic appendectomy is under investigation
• Antibiotic vs No Antibiotic : APPAC III
29.
Non-operative management
• RandomizedControl Trial > Br J Surg. 16 May 2022;Volume 109(6):503–509, doi:org
/10.1093/bjs/znac086
• Antibiotics versus placebo in adults with CT-confirmed uncomplicated
acute appendicitis (APPAC III): randomized double-blind superiority trial
• Paulina Salminen , Suvi Sippola , Jussi Haijanen , Pia Nordström , Tuomo
Rantanen , Tero Rautio , Ville Sallinen , Eliisa Löyttyniemi , Saija Hurme , Ville
Tammilehto , Johanna Laukkarinen , Heini Savolainen , Sanna Meriläinen , Ari
Leppäniemi , Juha Grönroos
• In the APPAC III trial (66 patients), 87 (95 % CI 75-99) per cent for placebo and 97%
(92-100) of those tx with antibiotics were successfully treated without surgery within 10
days. The diff was not statistically significant, ( p= 0.142)
30.
CONCLUSION
• Uncomplicated appendicitis:surgery (preferably laparoscopic) remains gold standard,
but NOM is viable for select patients.
• Complicated cases: NOM + drainage followed by IA reduces morbidity.
• Personalized care: tailor management to patient age, comorbidities, and presentation.
• Future research needs:
Long-term outcomes of NOM vs. surgery.
Standardized protocols for IA and antibiotic regimens
• LMIC: Non-operative treatment for AA has not been widely adopted in LMIC
REFERENCES
• WSES Jerusalemguidelines for diagnosis and treatment of acute appendicitis- Salomone Di Saverio1* , Arianna Birindelli2, Micheal D. Kelly3,
Fausto Catena4, Dieter G. Weber5, Massimo Sartelli6, Michael Sugrue7, Mark De Moya8, Carlos Augusto Gomes9, Aneel Bhangu10,
Ferdinando Agresta11,Ernest E. Moore12, Kjetil Soreide13, Ewen Griffiths14, Steve De Castro15, Jeffry Kashuk16, Yoram Kluger17,Ari
Leppaniemi18, Luca Ansaloni19, Manne Andersson20, Federico Coccolini19, Raul Coimbra21, Kurinchi S. Gurusamy22, Fabio Cesare
Campanile23, Walter Biffl24, Osvaldo Chiara25, Fred Moore26,Andrew B. Peitzman27, Gustavo P. Fraga28, David Costa29, Ronald V. Maier30,
Sandro Rizoli31, Zsolt J Balogh32, Cino Bendinelli32, Roberto Cirocchi33, Valeria Tonini2, Alice Piccinini34, Gregorio Tugnoli34, Elio Jovine35,
Roberto Persiani36, Antonio Biondi37, Thomas Scalea38, Philip Stahel12, Rao Ivatury39, George Velmahos40 and Roland Andersson20
• https://emedicine.medscape.com/article/773895treatment#:~:text=Patients%20with%20a%20phlegmon%20or,with%20the%20catheter%20i
n%20place
• Dahiya, D.S.; Akram, H.; Goyal, A.; Khan, A.M.; Shahnoor, S.; Hassan, K.M.; Gangwani, M.K.; Ali, H.; Pinnam, B.S.M.; Alsakarneh, S.; et al.
Controversies and Future Directions in Management of Acute Appendicitis: An Updated Comprehensive Review. J. Clin. Med. 2024, 13,
3034. https://doi.org/ 10.3390/jcm1311303
• Abdullatif Mahyoub., et al. “Non-Operative, Open, and Laparoscopic Management of Non-Perforated Appendicitis in Adults”. EC Microbiology
16.1 (2020): 01-09
• Sabiston Text book of Surgery Chapter 50 page 1296.
• The CODA Collaborative, 2020. A Randomized Trial Comparing Antibiotics with Appendectomy for Appendicitis. N. Engl. J. Med. 383 1907–
1919. https://doi.org/10.1056/NEJMoa2014320
• Talan, D.A., Saverio, S.D., 2021. Treatment of Acute Uncomplicated Appendicitis. N. Engl. J. Med. 385, 1116–1123.
https://doi.org/10.1056/NEJMcp2107675
• Dahiya, D.S., Akram, H., Goyal, A., Khan, A.M., Shahnoor, S., Hassan, K.M., Gangwani, M.K., Ali, H., Pinnam, B.S.M., Alsakarneh, S.,
Canakis, A., Sheikh, A.B., Chandan, S., Sohail, A.H., 2024. Controversies and Future Directions in Management of Acute Appendicitis: An
Updated Comprehensive Review. J. Clin. Med. 13, 3034. https://doi.org/10.3390/jcm13113034
Editor's Notes
#3 For over a century , open appendicetomy …..
laparoscopic appendectomy has surpassed open appendectomy
,initial antibiotic therapy followed by interval appendectomy for Perf AA
several trials suggested-its feasible to treat uncomplicated appendicitis nonoperatively with antibiotics alone
-In the current literature numerous knowledge gaps exist …..these include decisions on management
Optimal timing of Appendicectomy, Pre-operative Medicines
- Type of surgical intervention in high-risk populations (open versus/laparoscopic)
- Indications and timing of Interval Appendicectomy (IA)
- Need for drain placement
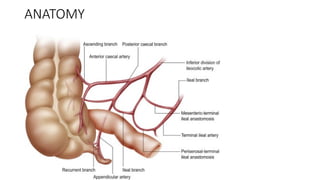
#4 The appendix is intraperitoneal and retrocecal(64%) in location, but it can be pelvic (32%), pre ileal, post ileal and subcecal.
#6 localized appendicitis without physical findings of diffuse peritonitis or imaging evidence of large abscess, phlegmon, perforation, or tumor
#7 Patients with suspected appendicitis should not receive anything by mouth.
IVF-SMART trial Lactated Ringers
3. Historically, analgesia critisized? render Physical exam less reliable however randomized controlled studies have demonstrated that administering opioid CARBAPENEMS/PENICILLINS /Cephalosporins
analgesic medications to adult and pediatric patients with acute undifferentiated abdominal pain is safe; no study has shown that analgesics adversely affect the accuracy of physical examination. 5.Preoperative antibiotics have demonstrated efficacy in decreasing postoperative wound infection rates in numerous prospective controlled studies, and they should be administered in conjunction with the surgical consultant.
#8 CODA and APPAC trials
Pregnancy: In pregnant women, management with antibiotic therapy alone is not recommended due to an increased risk of failure, a significant risk of fetal loss
with perforation, and a lack of sufficient safety data on this approach
Elderly/Immunocompromised: reduced immunity therefore late presentations with Higher perforation rates (55–70%); urgent surgery recommended
Indications for appendicectomy
- poor clinical response to conservative tx
- Deterioration on antibiotics
- Recurrent appendicitis
Success Rates:
90% resolve with antibiotics alone, but recurrence rates reach 15–40% within 1 year 24.
Meta-analyses show lower efficacy (73%) vs. surgery (98%)
#10 DELAY TRIAL: Of the 127 randomized participants, one group underwent immediate surgery (n = 68), while the delayed group (n = 59) had surgery postponed for an average duration of 11 h [39]. The comparison of outcomes revealed no significant differences between the two groups [39]. Essentially, the authors demonstrated the non-inferiority of postponing surgery until the following morning compared to immediate surgical intervention
potential of high-quality Computer Tomography (CT) imaging to predict the safety and feasibility of delaying appendectomy .
To conclude, appendectomy must be performed early after the initial resuscitation in patients with acute appendicitis.
#11 And provide coverage thus minimizing contamination risk: efficacy, cost, availability and route of administration
World Social of Emergency Surgery guidelines recommend the administration of a single dose of broad-spectrum antibiotics within 60 min of the surgical incision
#12 should wait for 24 hours (creatinine clearance >50 mL/min) to 48 hours (creatinine clearance ≤50 mL/min) from the last dose before undergoing appendectomyEvidence from the nonoperative management trials suggests that the rate of perforation is not higher as long as they are observed and receive antibiotics.,
receive vitamin K (2.5 to 5 mg oral or intravenous), which will reverse the warfarin in one to two days. Appendectomy can then proceed once the international normalized ratio (INR) value is normalized
#13 significant dehydration and electrolyte abnormalities, particularly if fever and vomiting have been present for a long time
Localize pain to right quadrant if walled off perforation
>4-6cms Antibiotics + drainage
< 4cm conservative management
#14 50% from highly populated residential areas, poor socioeconomic status, poor access to quality health care
33% wound infection
22% relaparatomies for intra-abd abscess
#15 Management depends on , pt hemodynamic stability, perf contained/free, mass/abscess
Unstable/free perf-emergency app either lap/open-immediate reversal of anticoagulants by giving inhibitors
Stable with mass/abscess –initial non operative management with antibiotics, intravenous fluids, and bowel rest and review after 6 weeks , rescue appendicectomy if failure
Immediate surgery ass with higher morbidity due to dense inflammation and adhesions , likely risk of injurying adjacent structures
FINNISH TRIAL-IA above 40 yr olds
any accessible abscess should be drained percutaneously under image guidance, drainage fewer Cxs and hospital stay allows inflammation to subside and negates appendicectomy need
the patient can be discharged with the catheter in place. Interval appendectomy can be performed after the fistula is closed.
Treatment failure, as evidenced by bowel obstruction, sepsis, or persistent pain, fever, or leukocytosis, requires immediate rescue appendectomy
If improvement of fever , Leucocytosis –introduce diet within 3-5 days
APPIC-antibiotic 2/5 days post complex appendicectomy
If the patient's symptoms, WBC count, and fever satisfactorily resolve, therapy can be changed to oral antibiotics and the patient can be discharged home. Then, delayed (interval) appendectomy can be performed 4-8 weeks later.
Risk if Neoplasm 12-28% in IA highest among > 40 yrs , reduced risk of recurrence
Against: rate of recurrence of symptoms after the successful NMO of perforated appendicitis is sufficiently low in asymptomatic patients
Some have suggested that interval appendectomy is not necessary, unless the patient presents with recurrent symptoms. Further studies are needed to clarify not only whether routine interval appendectomy is indicated but also to identify the optimal treatment strategy in patients with perforated appendicitis
#20 <3cm –appendicectomy
>3cm- per cutaneous drain and antibiotics
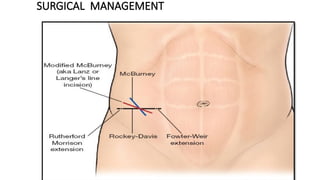
#23 Pt in supine position Incision choice is surgeon dependent/preference :
Oblique muscle splitting (McBurney)
Transverse (Rockey-Davis)
Lanz
Conservative Midline
Right lower paramedian incision/lower midline incision when in doubt or when there is diffuse peritonitis.
#24 According to the 2010 Society of American Gastrointestinal and Endoscopic Surgeons (SAGES) guideline, the indications for laparoscopic appendectomy are identical to those for open appendectomy. surgical advancement has led to laparoscopic appendectomy becoming the preferred intervention
#25 Advantages
o Diagnosis is confirmed.
o Other parts of the abdomen are visualised.
o In females pelvic structures are assessed properly.
o Trauma of access is less.
o Faster recovery.
o Laparoscopic appendicectomy is definitely better whenever there is vague abdominal pain; atypical pain; situs inversus; in women; subhepatic appendix and as interval appendicectomy.
may resolve with increasing experience with laparoscopic technique.
#26 Traditional teaching: prevent the collection of inflammatory debris, infection, blood, pus, and other fluids at the surgical site and aid in draining pre-existing collections
Because appendicectomy is associated with cxs likewound infections & intra abdominal infections/abscess
drain-associated complications like kinking etc
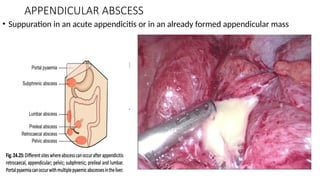
#27 Abscess sites : subphrenic,pelvic, retrocecal, preilieal, portam pyemia
persisting more than 4-5 days + fever , prompts further investigation
#29 Historically, for uncomplicated non-perforated appendicitis, the standard of care has been appendectomy owing to fear that untreated appendicitis leads to eventual perforation, thereby drastically increasing mortality risk. However, in recent years, the choice of treatment is dependent on several factors, including the presence of perforation or abscess, age, comorbidity profile, frailty, immune status, associated surgical risks, and the potential for appendiceal malignancy, among others.
The Appendicitis Acuta (APPAC) trial, which compared antibiotic therapy with appendectomy in the treatment of 530 patients with uncomplicated acute appendicitis confirmed by computed tomography (CT), was not able to demonstrate noninferiority of antimicrobial management versus surgery
Result-no significant difference in treatment success and major adverse effects between pts treated operatively vs nonoperatively for uncomplicated AA
However, those who received nonoperative management had a significantly longer length of hospital stay as well as a higher rate of recurrent appendicitis
Long term risk: the risk of needing appendicectomy returns to that of the general population.
#30 because of the diagnostic challenges of determining uncomplicated versus complicated appendicitis, the failure rate of non-operative management, and the consistently delayed presentation. In several LMICs, greater than 80% of the patients with AA present after 24 hours of symptoms




![APPENDICITIS Nursing managment[Autosaved].pptx](https://cdn.slidesharecdn.com/ss_thumbnails/appendicitisautosaved-250207063037-951fd6a3-thumbnail.jpg?width=640&height=640&fit=bounds)





































![Non-Communicable Diseases [Repaired].pptx](https://cdn.slidesharecdn.com/ss_thumbnails/non-communicablediseasesrepaired-240730032431-732c7df7-thumbnail.jpg?width=640&height=640&fit=bounds)












![PERI-PROSTHETIC FRACTURE NAIL-PLATE CONSTRUCT [NPC].pptx](https://cdn.slidesharecdn.com/ss_thumbnails/drarunkumardrmohamedashrafperiprostheticfrasturenail-plateconstructnpc-260209164459-7e9d15a1-thumbnail.jpg?width=640&height=640&fit=bounds)
![ONFH[AVN HIP] -TRIPLE REGIME -A NOVAL SURGICAL CONCEPT .pptx](https://cdn.slidesharecdn.com/ss_thumbnails/onfhavnhip2026koaconcalicutdrgokuldevdrmashraf-260210064517-213ec005-thumbnail.jpg?width=640&height=640&fit=bounds)








