Download to read offline
![DIAGNOSIS OF CANCER-ASSOCIATED ANEMIA
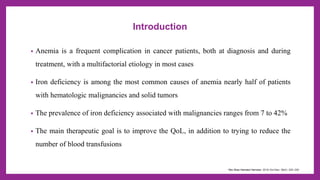
• Definition: We define anemia as cancer-associated anemia when it results from
malignancy or its treatment
• The most widely available and frequently used tests to assess iron status are
• Serum Ferritin & Transferrin Saturation (TSAT %)
• TSAT%= [ Serum iron / TIBC (Total iron binding capacity)] x 100
• Ferritin- acute phase reactant- may be falsely elevated in cancers
• Ferritin is a biomarker of total body iron stores, and low ferritin is a reliable indicator of
absolute iron deficiency
(Blood. 2020;136(7):801-813)](https://image.slidesharecdn.com/malignancyassocitaedanemia-231203005908-43d48981/85/Malignancy-Associtaed-Anemia-pptx-5-320.jpg)
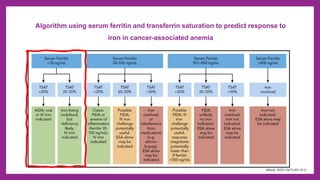
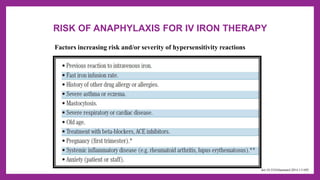



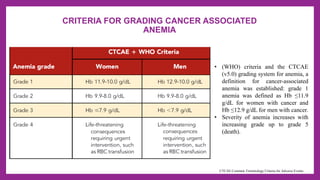
This document summarizes information on malignancy-associated anemia, including its prevalence, potential etiologies, diagnostic criteria, and treatment approaches. It discusses how anemia is common in cancer patients, often due to iron deficiency. The main goals of treatment are to improve quality of life and reduce blood transfusions. It provides algorithms for diagnosing and predicting response to iron therapy for cancer-associated anemia. Risks of intravenous iron therapy are addressed, along with strategies for risk minimization and managing potential hypersensitivity reactions. Monitoring of patients after IV iron treatment is also summarized.























































































